

Continued Investigation Into 17-OHPC: Results From the Preclinical RUPP Rat Model of Preeclampsia
- PMID: 29084881
- PMCID: PMC5901972
- DOI: 10.1161/HYPERTENSIONAHA.117.09969
Continued Investigation Into 17-OHPC: Results From the Preclinical RUPP Rat Model of Preeclampsia
Abstract
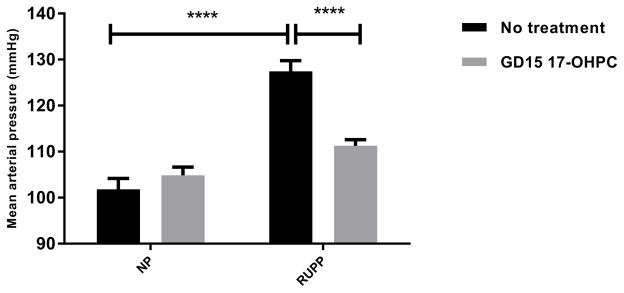
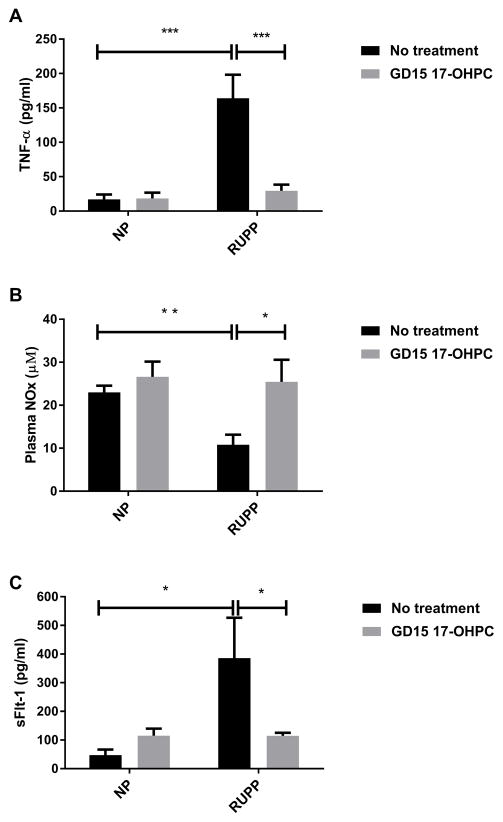
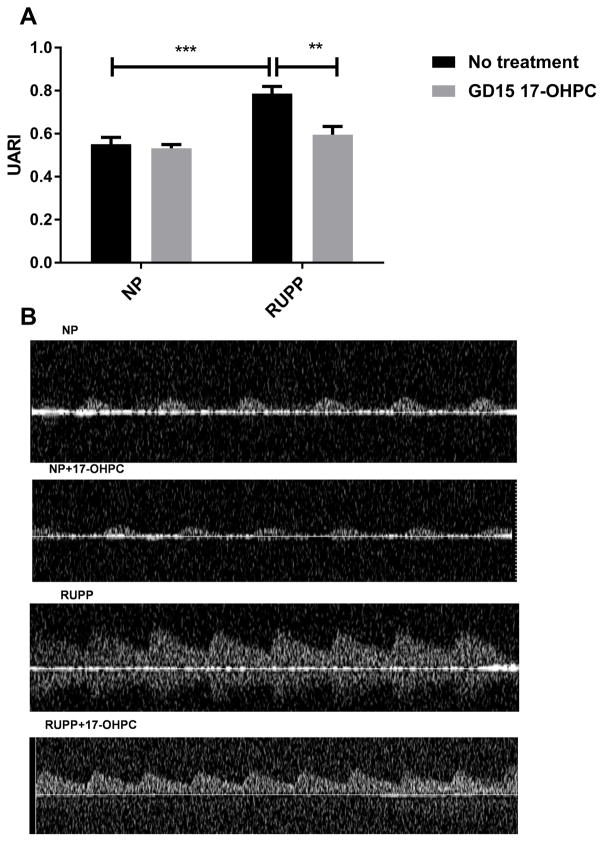
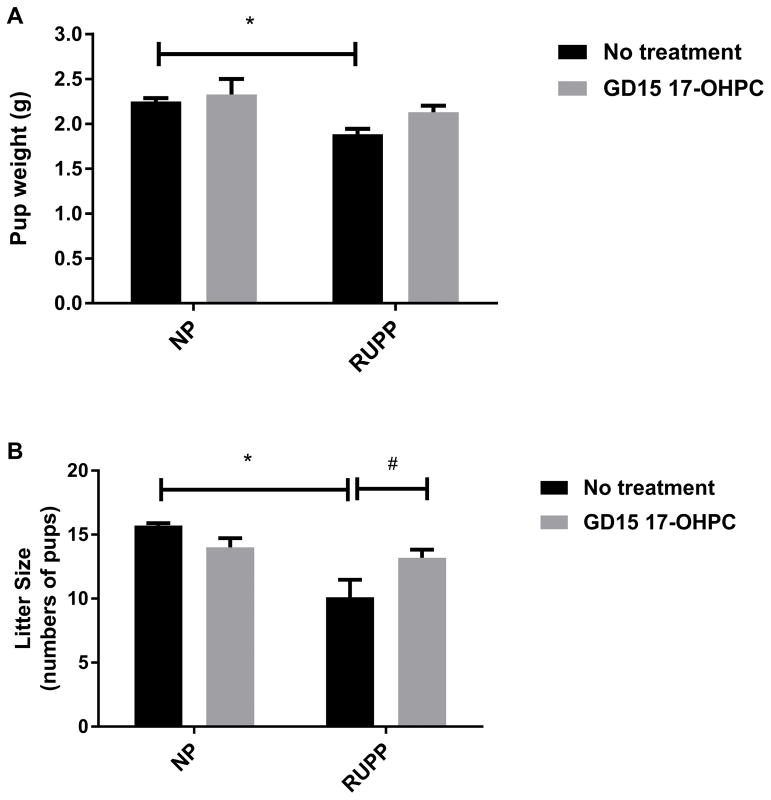
Preeclampsia is characterized by elevated TNF-α (tumor necrosis factor-α), antiangiogenic factors, such as sFlt-1 (soluble vascular endothelial growth factor receptor 1), increased uterine artery resistance index, and decreased of NO during pregnancy. Previously we showed that 17-hydroxyprogesterone caproate (17-OHPC) administered into reduced uterine perfusion pressure (RUPP) rats on day 18 of gestation improved hypertension without improving pup weight. We hypothesized that earlier administration of 17-OHPC on day 15 of gestation could improve pathophysiology of preeclampsia and fetal outcomes in response to placental ischemia. Carotid catheters were inserted on day 18, and mean arterial blood pressure and samples were collected on day 19. Mean arterial blood pressure in normal pregnant rats was 102±2, 105±2 in normal pregnant+day 15 of gestation (GD15) 17-OHPC, 127±2 in RUPP and 112±1 mm Hg in RUPP+GD15 17-OHPC, P<0.05. Pup weight and litter size were improved from 1.9±0.05, 10.1±1.4 in RUPP to 2.1±0.07 g and 13.2±0.6 in RUPP+GD15 17-OHPC, P<0.05. Uterine artery resistance index was 0.8±0.03 in RUPP, which was decreased to 0.6±0.04 in RUPP+GD15 17-OHPC, P<0.05. Plasma TNF-α levels were 164±34 in RUPP and blunted to 29±9 pg/mL in RUPP+GD15 17-OHPC, P<0.05. Plasma nitrate-nitrite levels were 10.8±2.3 in RUPP rats and significantly increased to 25.5±5.2 µmol/L in RUPP+GD15 17-OHPC, P<0.05. sFlt-1 levels were 386±141 in RUPP rats, which were reduced to 110.2±11 in RUPP+17-OHPC, P<0.05. These data indicate that GD15 17-OHPC improves pathophysiology in RUPP rats, possibly via improving sFlt-1 reduced NO during pregnancy.
Keywords: humans; inflammation; nitric oxide; preeclampsia; pregnancy.
© 2017 American Heart Association, Inc.
Figures
References
-
- World health organization. [Acessed february 6, 2015];Maternal mortality fact sheet no. 348. 2012 Available from: http://www.Who.Int/mediacentre/factsheets/fs348/en/
-
- Noris M, Perico N, Remuzzi G. Mechanisms of disease: Pre-eclampsia. Nature clinical practice. Nephrology. 2005;1:98–114. quiz 120. - PubMed
-
- Sibai B, Dekker G, Kupferminc M. Pre-eclampsia. Lancet. 2005;365:785–799. - PubMed
-
- Granger JP, Alexander BT, Llinas MT, Bennett WA, Khalil RA. Pathophysiology of preeclampsia: Linking placental ischemia/hypoxia with microvascular dysfunction. Microcirculation. 2002;9:147–160. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
