

Redifferentiation of Radioiodine Refractory Differentiated Thyroid Cancer for Reapplication of I-131 Therapy
- PMID: 29085335
- PMCID: PMC5649198
- DOI: 10.3389/fendo.2017.00260
Redifferentiation of Radioiodine Refractory Differentiated Thyroid Cancer for Reapplication of I-131 Therapy
Abstract
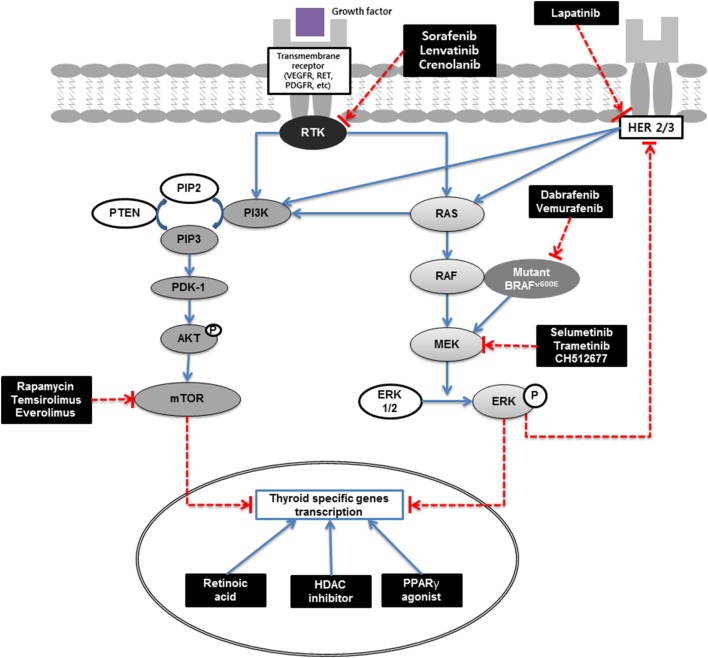
Although most differentiated thyroid cancers show excellent prognosis, treating radioiodine refractory differentiated thyroid cancer (RR-DTC) is challenging. Various therapies, including chemotherapy, radiotherapy, and targeted therapy, have been applied for RR-DTC but show limited effectiveness. Redifferentiation followed by radioiodine therapy is a promising alternative therapy for RR-DTC. Retinoic acids, histone deacetylase inhibitors, and peroxisome proliferator-activated receptor-gamma agonists are classically used as redifferentiation agents, and recent targeted molecules are also used for this purpose. Appropriate selection of redifferentiation agents for each patient, using current knowledge about genetic and biological characteristics of thyroid cancer, might increase the efficacy of redifferentiation treatment. In this review, we will discuss the mechanisms of these redifferentiation agents, results of recent clinical trials, and promising preclinical results.
Keywords: I-131; NIS; differentiated thyroid cancer; radioiodine refractory; redifferentiation.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources