

Bronchial Wash Gene Xpert MTB/RIF in Lower Lung Field Tuberculosis: Sensitive, Superior, and Rapid in Comparison with Conventional Diagnostic Techniques
- PMID: 29085791
- PMCID: PMC5655465
- DOI: 10.1515/jtim-2017-0030
Bronchial Wash Gene Xpert MTB/RIF in Lower Lung Field Tuberculosis: Sensitive, Superior, and Rapid in Comparison with Conventional Diagnostic Techniques
Abstract
Background: Lower lung field tuberculosis (LLF TB) is an atypical presentation of tuberculosis (TB). LLF TB is common, and a proportionate number of non-resolving pneumonia cases are diagnosed to have pulmonary TB.
Materials and methods: The prospective observational study was conducted during June 2013 to December 2015 in the Department of Pulmonary Medicine, MIMSR Medical College, Latur, India; the objective of the study is clinical, microbiological, and radiological presentation of LLF TB and the comparison of yield of conventional diagnostic techniques and bronchoscopy-guided modalities in LLF TB. Additional important objective of the study is to find LLF TB in patients with nonresolving pneumonia (NRP). A total of 2,600 patients with pulmonary TB were included in the study after inclusion and exclusion criteria. Ethical clearance was taken from the ethical committee of the institutional review board. Consent was taken from the patients before inclusion in the study. Statistical analysis was done using chi-square test.
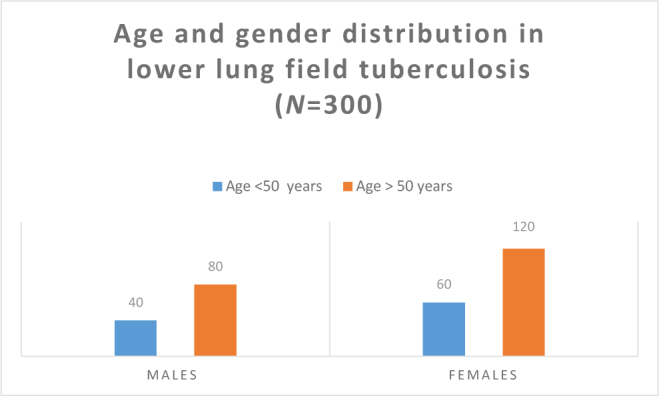
Results: In the present study, 300 (11.53%) cases of LLF TB of total 2600 pulmonary tuberculosis were included, females constitutes 66.66% (200/300) with mean age of 58.4 ± 11.8 years and males constitutes 33.34% (100/300) with mean age of 56.8 ± 10.6 years. Constitutional symptoms were observed as cough in 93% cases, fever in 83% cases, shortness of breath in 72% cases, anorexia in 91% cases, and weight loss in 84% cases. Radiological assessment of study cases documented the involvement of right lower zone in 84% cases and left lower zone in only 16% cases. In the studied LLF TB cases, 57 cases (20.66%) were diagnosed by routine sputum microscopic examination for acid fast bacilli (AFB) and 80 cases (28%) were diagnosed by induced sputum microscopic examination for AFB. In the study of 170 LLF TB cases, head-to-head comparison between conventional diagnostic techniques (sputum microscopy and Induced sputum microscopy for AFB) made diagnosis in 60 cases, while bronchoscopy-guided sampling techniques (BAL for AFB and BAL for Gene Xpert MTB/RIF) made diagnosis in 155 cases (91.17%) (P < 0.00001). Comorbid conditions such as human immunodeficiency virus (HIV) coinfection in 36 cases (12.00%), Diabetes mellitus in 64 cases (21.33%), and chronic kidney disease (CKD) in 22 cases (7.33%) were observed. Comorbidities were observed in 41.67% of the studied cases and found very significant assessment to have successful treatment outcome (P < 0.00001). In the study of 300 LLF TB cases, 60 cases were having NRP pattern. In LLF TB cases with NRP pattern, bronchoscopy-guided bronchial wash microscopy for AFB made diagnosis in 18 cases (42%), while bronchoscopy-guided BAL for Gene Xpert MTB/RIF made diagnosis in 58 cases (96.66%) (P < 0.00001).
Conclusion: LLF TB is usually underdiagnosed because of diverse clinical and radiological presentation, less diagnostic yield of conventional diagnostic modalities, and these modalities used routinely and universally. Bronchoscopy-guided diagnostic techniques are superior, sensitive, and reliable to confirm LLF TB. Gene Xpert MTB/RIF in bronchial wash samples is found to be best diagnostic modality in evaluating LLF TB and should be used routinely to have successful treatment outcome. A proportionate number of NRP cases are having LLF TB and a high index of suspicion is a must while evaluating these cases.
Keywords: BAL Gene Xpert MTB/RIF; bronchoscopy; lower lung field tuberculosis (LLF TB); treatment outcome.
Conflict of interest statement
Conflict of Interest: None declared.
Figures
References
-
- WHO, Tuberculosis. WHO. 2015 http://www.who.int/mediacentre/factsheets/fs104/en/ Available from.
-
- Greenberg SD, Frager D, Suster B, Walker S, Stavropoulos C, Rothpearl A. et al. Active pulmonary tuberculosis in patients with AIDS: Spectrum of radiographic findings (including a normal appearance) Radiology. 1994;193:115–9. - PubMed
-
- Segarra F, Sherman DS, Rodriguez-Aguem J. Lower lung field tuberculosis. Am Rev Resp Dis. 1963:8737–40. - PubMed
-
- Ossen EZ. Tuberculosis of the lower lobe. N Engl J Med. 1844;230:693–8.
-
- Andosca JB, Foley JA. Basal tuberculosis. J Thorac Surg. 1943;12:259–66.
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous