

Pathophysiology of Hyponatremia in Children
- PMID: 29085814
- PMCID: PMC5650627
- DOI: 10.3389/fped.2017.00213
Pathophysiology of Hyponatremia in Children
Abstract
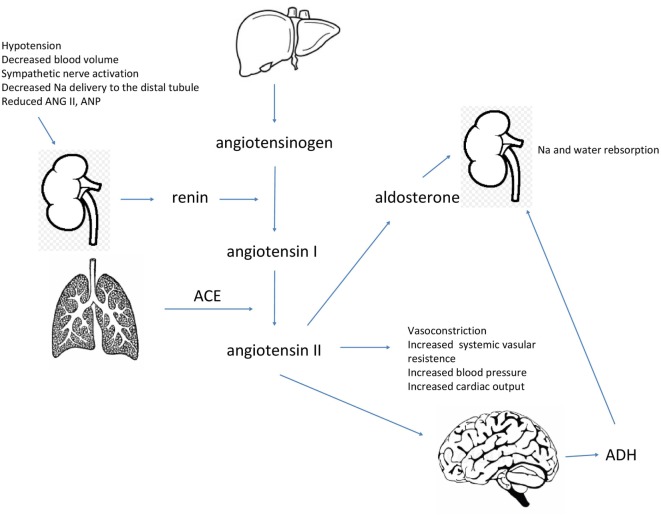
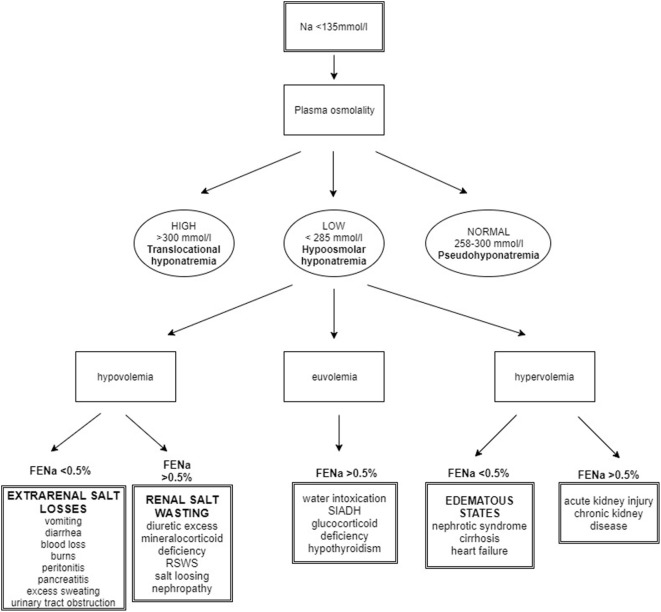
Hyponatremia is a common electrolyte disorder in children. It is generally defined as plasma sodium of less than 135 mmol/l. Sodium homeostasis is essential for maintaining intravascular volume and is tightly linked to water balance. Plasma water volume is regulated mainly by the secretion of an antidiuretic hormone (ADH) and by the thirst mechanism. ADH is synthesized in the hypothalamus and stored in the posterior hypophysis. It binds to V2 receptors in the distal nephron and induces translocation of aquaporin water channels in the plasma membrane to retain water. There are two main types of receptors involved in the control of the body water balance-osmoreceptors and baroreceptors. Osmoreceptors reside in hypothalamus and respond to changes of extracellular fluid (ECF) osmolality. Baroreceptors are mechanoreceptors that sense blood pressure in the vessel wall. Response reflexes from baroreceptors influence sympathetic outflow, vessel tonus, and cardiac output. An increase of 1% of plasma osmolality may cause an increase in ADH levels, while the threshold of volume receptors for ADH secretion is higher. However, significant hypotension is a more potent stimulus for ADH secretion than increased osmolality. The main cause of pediatric hyponatremia is an abundance of free water. This may occur in hypovolemic children with low ECF volume, normovolemic patients with inappropriately increased ADH secretion, and also in hypervolemic individuals with decreased effective circulating volume and appropriately increased ADH levels. Proper understanding of the pathophysiology of hyponatremic states is essential for establishing the correct diagnosis and appropriate therapy.
Keywords: antidiuretic hormone; baroreceptor; children; hyponatremia; osmoreceptor; pathophysiology.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources