

Clinical Pharmacokinetic and Pharmacodynamic Profile of Riociguat
- PMID: 29086344
- PMCID: PMC5974002
- DOI: 10.1007/s40262-017-0604-7
Clinical Pharmacokinetic and Pharmacodynamic Profile of Riociguat
Abstract
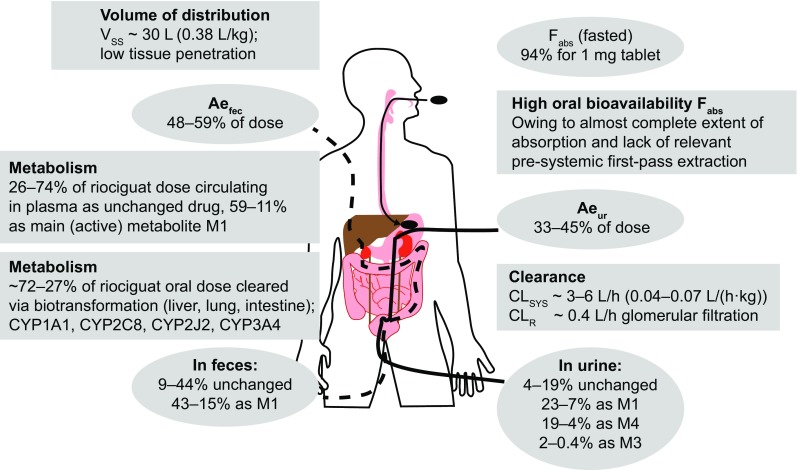
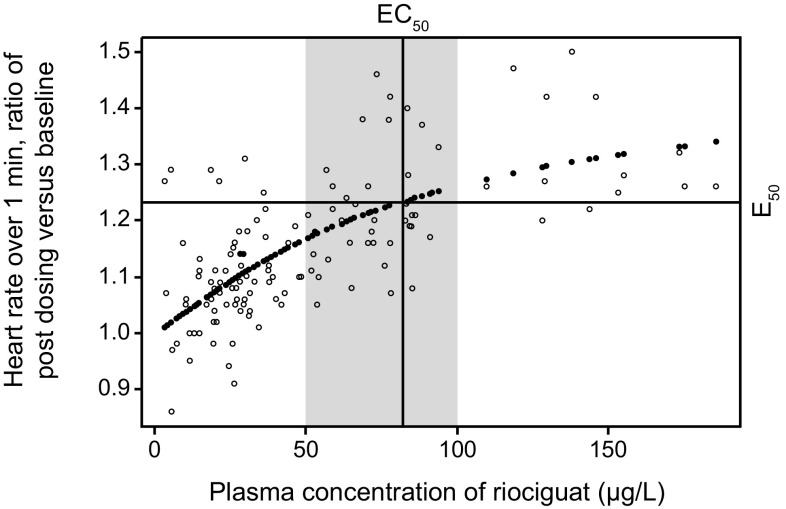
Oral riociguat is a soluble guanylate cyclase (sGC) stimulator that targets the nitric oxide (NO)-sGC-cyclic guanosine monophosphate pathway with a dual mode of action: directly by stimulating sGC, and indirectly by increasing the sensitivity of sGC to NO. It is rapidly absorbed, displays almost complete bioavailability (94.3%), and can be taken with or without food and as crushed or whole tablets. Riociguat exposure shows pronounced interindividual (60%) and low intraindividual (30%) variability in patients with pulmonary arterial hypertension (PAH) or chronic thromboembolic pulmonary hypertension (CTEPH), and is therefore administered using an individual dose-adjustment scheme at treatment initiation. The half-life of riociguat is approximately 12 h in patients and approximately 7 h in healthy individuals. Riociguat and its metabolites are excreted via both renal (33-45%) and biliary routes (48-59%), and dose adjustment should be performed with particular care in patients with moderate hepatic impairment or mild to severe renal impairment (no data exist for patients with severe hepatic impairment). The pharmacodynamic effects of riociguat reflect the action of a vasodilatory agent, and the hemodynamic response to riociguat correlated with riociguat exposure in patients with PAH or CTEPH in phase III population pharmacokinetic/pharmacodynamic analyses. Riociguat has a low risk of clinically relevant drug interactions due to its clearance by multiple cytochrome P450 (CYP) enzymes and its lack of effect on major CYP isoforms and transporter proteins at therapeutic levels. Riociguat has been approved for the treatment of PAH and CTEPH that is inoperable or persistent/recurrent after surgical treatment.
Conflict of interest statement
Funding
Support for the preparation of this manuscript was provided by Bayer AG.
Conflict of interest
Reiner Frey is a former employee of, and now a consultant to, Bayer AG. Corina Becker, Soundos Saleh, Sigrun Unger, Dorina van der Mey, and Wolfgang Mück are employees of Bayer AG. Reiner Frey, Sigrun Unger, and Wolfgang Mück own stock in Bayer.
Figures
References
-
- Galiè N, Humbert M, Vachiery JL, Gibbs S, Lang I, Torbicki A, et al. 2015 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension: The joint task force for the diagnosis and treatment of pulmonary hypertension of the European Society of Cardiology (ESC) and the European Respiratory Society (ERS): Endorsed by: Association for European Paediatric and Congenital Cardiology (AEPC), International Society for Heart and Lung Transplantation (ISHLT) Eur Respir J. 2015;46(4):903–975. doi: 10.1183/13993003.01032-2015. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
