

Differential responses to larger volume intra-aortic balloon counterpulsation: Hemodynamic and clinical outcomes
- PMID: 29086475
- PMCID: PMC6221162
- DOI: 10.1002/ccd.27387
Differential responses to larger volume intra-aortic balloon counterpulsation: Hemodynamic and clinical outcomes
Abstract
Objectives: Examine hemodynamic and clinical correlates of use of an intra-aortic balloon pump catheter in a single center.
Background: The intra-aortic balloon pump catheter (IABC) has been used for 50 years but the clinical benefit is still debated. We reviewed 76 patients with right heart catheter measurements prior to IABC to assess response and outcomes.
Methods: All patients who received IABC with a 50cc balloon for at least 1 hour were included in this retrospective chart review study. Demographics, comorbidities, lab values, and hemodynamic parameters were recorded at baseline and 15 h postinsertion.
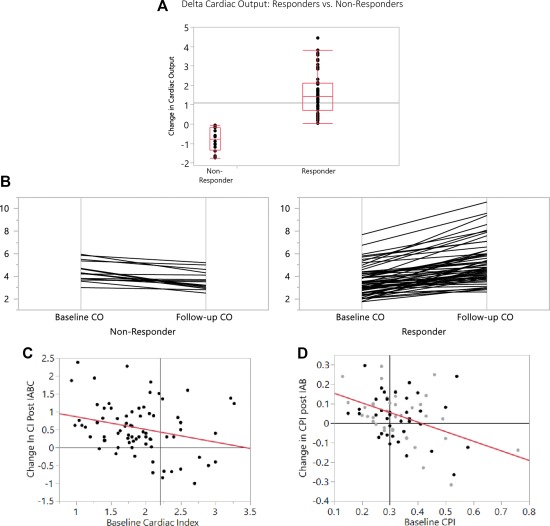
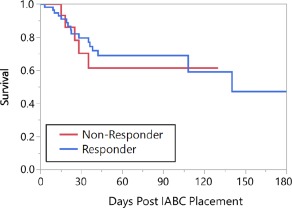
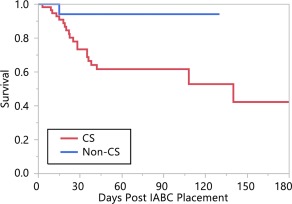
Results: Seventy-six patients had paired measurements of cardiac output. 60 patients had a higher cardiac output with IABC treatment (responder group) and 16 did not (nonresponders). In the 60 patients in the responder group, cardiac output and index significantly increased from baseline 3.6 ± 1.3 L/min to 5.2 ± 1.8 L/min, and 1.8 ± 0.5 L/min/m2 to 2.6 ± 0.8 L/min/m2 respectively following IABC placement (P < 0.0001 for both comparisons). Various hemodynamic variables were examined and the best predictor of response to IABC was a cardiac power index of 0.3 or less. Regardless of response, in hospital survival was similar between groups.
Conclusions: The majority of patients improve their cardiac output with IABC but survival was unchanged. Further work into the pathophysiology of cardiogenic shock is needed.
Keywords: cardiogenic shock; counterpulsation; mortality; systolic heart failure.
© 2017 The Authors Catheterization and Cardiovascular Interventions Published by Wiley Periodicals, Inc.
Figures
Comment in
-
Counterpulsation requires pulsation: IABP use in patients with heart failure without acute MI.Catheter Cardiovasc Interv. 2018 Oct 1;92(4):711-712. doi: 10.1002/ccd.27878. Catheter Cardiovasc Interv. 2018. PMID: 30341827
Similar articles
-
Acute Mechanical Circulatory Support for Cardiogenic Shock.Methodist Debakey Cardiovasc J. 2020 Jan-Mar;16(1):27-35. doi: 10.14797/mdcj-16-1-27. Methodist Debakey Cardiovasc J. 2020. PMID: 32280415 Free PMC article. Review.
-
A single center tertiary care experience utilizing the large volume mega 50cc intra-aortic balloon counterpulsation in contemporary clinical practice.Catheter Cardiovasc Interv. 2017 Oct 1;90(4):E63-E72. doi: 10.1002/ccd.26908. Epub 2017 Feb 1. Catheter Cardiovasc Interv. 2017. PMID: 28145044
-
The hemodynamic response to intra-aortic balloon counterpulsation in patients with cardiogenic shock complicating acute myocardial infarction.Am Heart J. 1977 Mar;93(3):274-9. doi: 10.1016/s0002-8703(77)80244-5. Am Heart J. 1977. PMID: 842426
-
Effective arterial elastance and the hemodynamic effects of intraaortic balloon counterpulsation in patients with coronary heart disease.Am Heart J. 1998 May;135(5 Pt 1):855-61. doi: 10.1016/s0002-8703(98)70046-8. Am Heart J. 1998. PMID: 9588417 Clinical Trial.
-
Balloon Pump Counterpulsation Part II: Perioperative Hemodynamic Support and New Directions.Anesth Analg. 2020 Sep;131(3):792-807. doi: 10.1213/ANE.0000000000004999. Anesth Analg. 2020. PMID: 32665471 Review.
Cited by
-
Utility of Cardiac Power Hemodynamic Measurements in the Evaluation and Risk Stratification of Cardiovascular Conditions.Healthcare (Basel). 2022 Nov 30;10(12):2417. doi: 10.3390/healthcare10122417. Healthcare (Basel). 2022. PMID: 36553940 Free PMC article. Review.
-
Intra-aortic balloon pump postcardiac surgery: A literature review.J Res Med Sci. 2019 Jan 31;24:6. doi: 10.4103/jrms.JRMS_199_18. eCollection 2019. J Res Med Sci. 2019. PMID: 30815019 Free PMC article. Review.
-
Mechanical Support in Early Cardiogenic Shock: What Is the Role of Intra-aortic Balloon Counterpulsation?Curr Heart Fail Rep. 2020 Oct;17(5):247-260. doi: 10.1007/s11897-020-00480-0. Curr Heart Fail Rep. 2020. PMID: 32870448 Free PMC article. Review.
-
Acute Mechanical Circulatory Support for Cardiogenic Shock.Methodist Debakey Cardiovasc J. 2020 Jan-Mar;16(1):27-35. doi: 10.14797/mdcj-16-1-27. Methodist Debakey Cardiovasc J. 2020. PMID: 32280415 Free PMC article. Review.
-
Intra-aortic Balloon Counterpulsation for High-Risk Percutaneous Coronary Intervention: Defining Coronary Responders.J Cardiovasc Transl Res. 2019 Aug;12(4):299-309. doi: 10.1007/s12265-019-09871-8. Epub 2019 Mar 15. J Cardiovasc Transl Res. 2019. PMID: 30877563 Free PMC article.
References
-
- Visveswaran GK, Cohen M, Seliem A, DiVita M, McNamara JK, Dave A, et al. A single center tertiary care experience utilizing the large volume mega 50cc intra‐aortic balloon counterpulsation in contemporary clinical practice. Cathet Cardiovasc Interv 2017;90:E63–E72. - PubMed
-
- Seyfarth M, Sibbing D, Bauer I, Frohlich G, Bott‐Flugel L, Byrne R, et al. A randomized clinical trial to evaluate the safety and efficacy of a percutaneous left ventricular assist device versus intra‐aortic balloon pumping for treatment of cardiogenic shock caused by myocardial infarction. J Am Coll Cardiol 2008;52:1584–1588. - PubMed
-
- Thiele H, Sick P, Boudriot E, Diederich KW, Hambrecht R, Niebauer J, et al. Randomized comparison of intra‐aortic balloon support with a percutaneous left ventricular assist device in patients with revascularized acute myocardial infarction complicated by cardiogenic shock. Eur Heart J 2005;26:1276–1283. - PubMed
-
- Fincke R, Hochman JS, Lowe AM, Menon V, Slater JN, Webb JG, et al. Cardiac power is the strongest hemodynamic correlate of mortality in cardiogenic shock: a report from the SHOCK trial registry. J Am Coll Cardiol 2004;44:340–348. - PubMed
-
- Rigamonti F, Graf G, Merlani P, Bendjelid K. The short‐term prognosis of cardiogenic shock can be determined using hemodynamic variables: a retrospective cohort study*. Crit Care Med 2013;41:2484–2491. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
