

46-Year Trends in Systemic Lupus Erythematosus Mortality in the United States, 1968 to 2013: A Nationwide Population-Based Study
- PMID: 29086801
- PMCID: PMC6188647
- DOI: 10.7326/M17-0102
46-Year Trends in Systemic Lupus Erythematosus Mortality in the United States, 1968 to 2013: A Nationwide Population-Based Study
Abstract
Background: No large population-based studies have been done on systemic lupus erythematosus (SLE) mortality trends in the United States.
Objective: To identify secular trends and population characteristics associated with SLE mortality.
Design: Population-based study using a national mortality database and census data.
Setting: United States.
Participants: All U.S. residents, 1968 through 2013.
Measurements: Joinpoint trend analysis of annual age-standardized mortality rates (ASMRs) for SLE and non-SLE causes by sex, race/ethnicity, and geographic region; multiple logistic regression analysis to determine independent associations of demographic variables and period with SLE mortality.
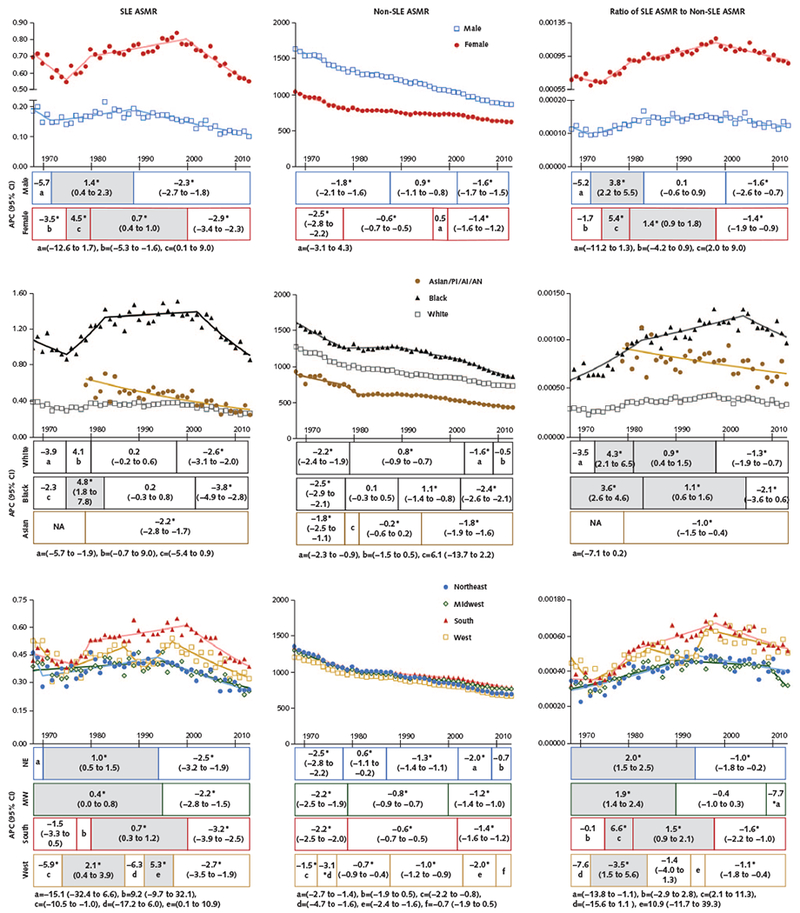
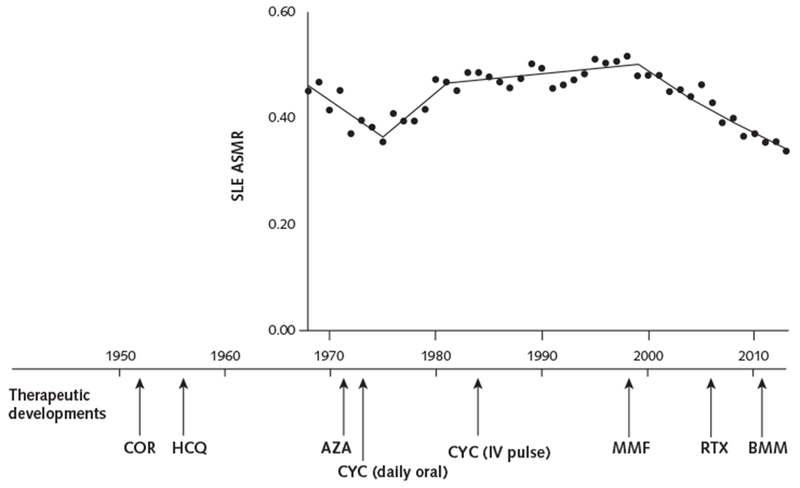
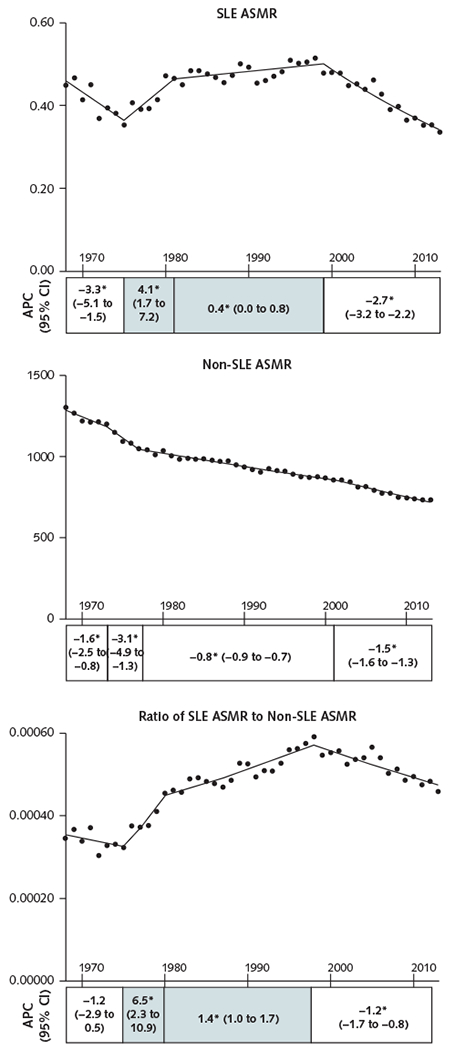
Results: There were 50 249 SLE deaths and 100 851 288 non-SLE deaths from 1968 through 2013. Over this period, the SLE ASMR decreased less than the non-SLE ASMR, with a 34.6% cumulative increase in the ratio of the former to the latter. The non-SLE ASMR decreased every year starting in 1968, whereas the SLE ASMR decreased between 1968 and 1975, increased between 1975 and 1999, and decreased thereafter. Similar patterns were seen in both sexes, among black persons, and in the South. However, statistically significant increases in the SLE ASMR did not occur among white persons over the 46-year period. Females, black persons, and residents of the South had higher SLE ASMRs and larger cumulative increases in the ratio of the SLE to the non-SLE ASMR (31.4%, 62.5%, and 58.6%, respectively) than males, other racial/ethnic groups, and residents of other regions, respectively. Multiple logistic regression showed independent associations of sex, race, and region with SLE mortality risk and revealed significant racial/ethnic differences in associations of SLE mortality with sex and region.
Limitations: Underreporting of SLE on death certificates may have resulted in underestimates of SLE ASMRs. Accuracy of coding on death certificates is difficult to ascertain.
Conclusion: Rates of SLE mortality have decreased since 1968 but remain high relative to non-SLE mortality, and significant sex, racial, and regional disparities persist.
Primary funding source: None.
Conflict of interest statement
Figures
References
Web-Only References
-
- Mullins JF, Watts FL, Wilson CJ. Plaquenil in the treatment of lupus erythematosus. J Am Med Assoc 1956;161:879–81. [PMID: ] - PubMed
-
- Johnson SA, Meyer OO. The treatment of lupus erythematosus disseminatus with cortisone. Am J Med Sci 1952;223:9–15. [PMID: ] - PubMed
-
- Sztejnbok M, Stewart A, Diamond H, Kaplan D. Azathioprine in the treatment of systemic lupus erythematosus. A controlled study. Arthritis Rheum 1971;14:639–45. [PMID: ] - PubMed
-
- Felson DT, Anderson J Evidence for the superiority of immunosuppressive drugs and prednisone over prednisone alone in lupus nephritis. Results of a pooled analysis. N Engl J Med 1984;311: 1528–33. [PMID: ] - PubMed
-
- National Cancer Institute. Joinpoint Help Manual 4.5.0.1. Bethesda: National Cancer Institute; Accessed at https://surveillance.cancer.gov/joinpoint/Joinpoint_Help_4.5.0.1.pdf on 3 October 2017.
References
-
- Singh RR. Systemic lupus erythematosus In: Madhok R, Luthra H, eds. The Year in Rheumatic Disorders. Oxford, United Kingdom: Atlas Medical Publishing; 2007:171–90.
-
- Cervera R, Khamashta MA, Font J, Sebastiani GD, Gil A, Lavilla P, et al. ; European Working Party on Systemic Lupus Erythematosus. Morbidity and mortality in systemic lupus erythematosus during a 10-year period: a comparison of early and late manifestations in a cohort of 1,000 patients. Medicine (Baltimore). 2003;82:299–308. [PMID: ] - PubMed
-
- Bernatsky S, Boivin JF, Joseph L, Manzi S, Ginzler E, Gladman DD, et al. Mortality in systemic lupus erythematosus. Arthritis Rheum 2006;54:2550–7. [PMID: ] - PubMed
-
- Urowitz MB, Gladman DD, Tom BD, Ibanez D, Farewell VT. Changing patterns in mortality and disease outcomes for patients with systemic lupus erythematosus. J Rheumatol 2008;35:2152–8. [PMID: ] - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical