

Underutilization of Statins When Indicated in HIV-Seropositive and Seronegative Women
- PMID: 29087746
- PMCID: PMC5665094
- DOI: 10.1089/apc.2017.0145
Underutilization of Statins When Indicated in HIV-Seropositive and Seronegative Women
Abstract
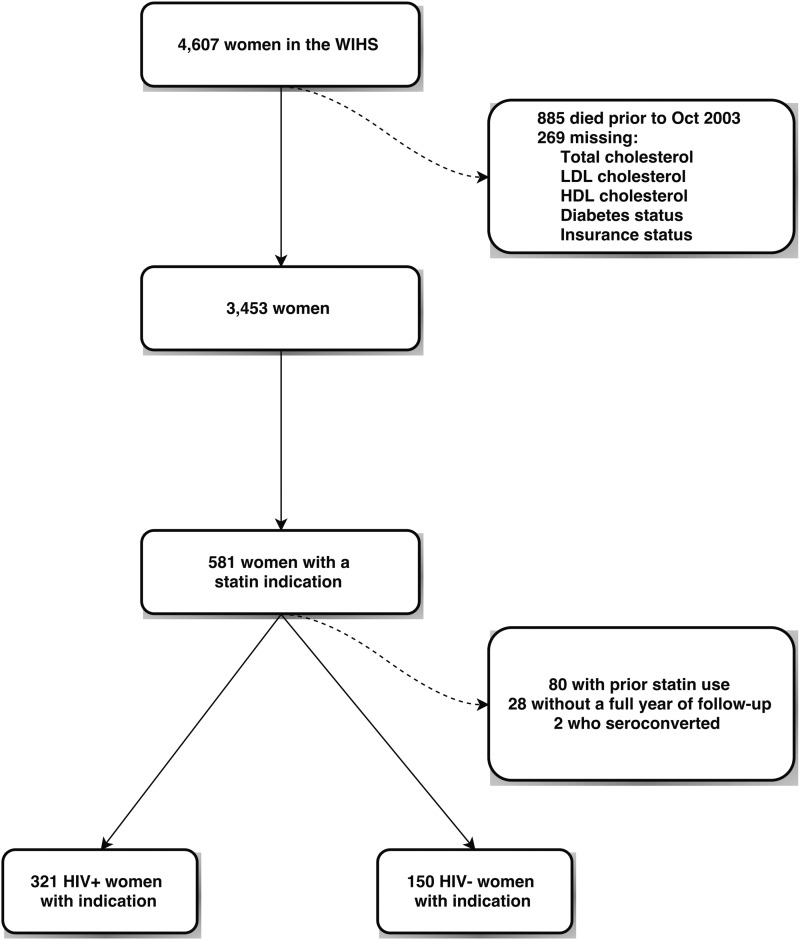
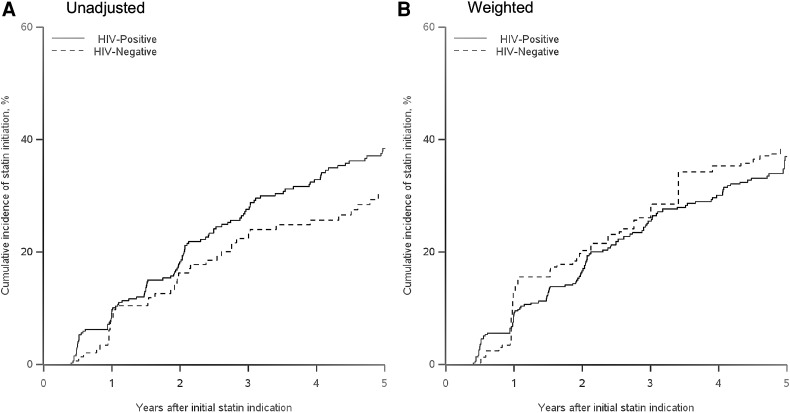
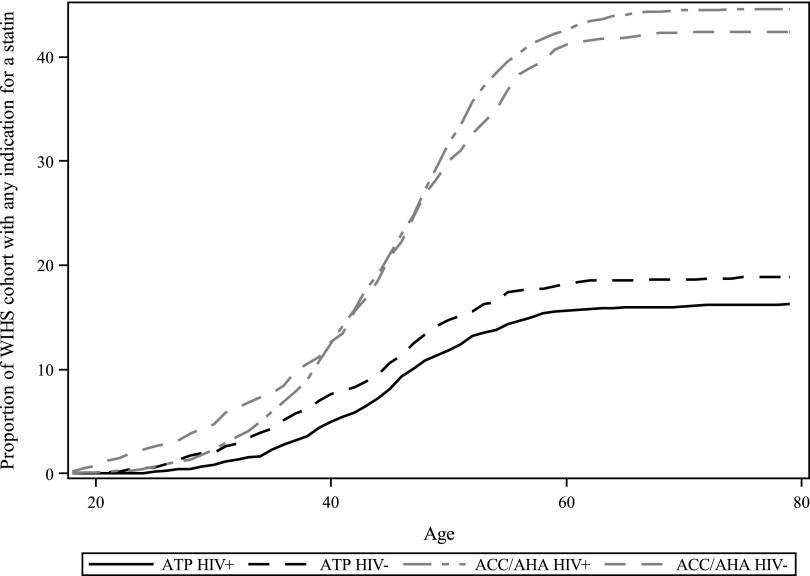
Increased life expectancy of persons living with HIV infection receiving antiretroviral therapy heightens the importance of preventing and treating chronic comorbidities such as cardiovascular disease. While guidelines have increasingly advocated more aggressive use of statins for low-density lipoprotein (LDL) cholesterol reduction, it is unclear whether people with HIV, especially women, are receiving statins when indicated, and whether their HIV disease is a factor in access. We assessed the cumulative incidence of statin use after an indication in the Women's Interagency HIV Study (WIHS), from 2000 to 2014. Additionally, we used weighted proportional hazards regression to estimate the effect of HIV serostatus on the time to initiation of a statin after an indication. Cumulative incidence of statin use 5 years after an indication was low: 38% in HIV-seropositive women and 30% in HIV-seronegative women. Compared to HIV-seronegative women, the weighted hazard ratio for initiation of a statin for HIV-seropositive women over 5 years was 0.94 [95% confidence interval (CI) 0.62, 1.43]. Applying the American College of Cardiology and the American Heart Association (ACC/AHA) guidelines increased the proportion of HIV-seropositive women with a statin indication from 16% to 45%. Clinicians treating HIV-seropositive women should consider more aggressive management of the dyslipidemia often found in this population.
Keywords: cardiovascular disease; human immunodeficiency virus; hydroxymethylglutaryl-CoA reductase inhibitors; lipids; statins; women's health.
Conflict of interest statement
M.J.F. is a member of the Scientific Steering Committee (SSC) for a postapproval safety study funded by GlaxoSmithKline, and receives salary support through a contract with AstraZeneca. G.B. has research support from Amgen, Inc., Bristol-Myers Squibb, and has consulted for Definicare, LLC. All other authors have no potential conflicts of interest to disclose.
Figures
References
-
- Dubé MP, Stein JH, Aberg JA, et al. Guidelines for the evaluation and management of dyslipidemia in human immunodeficiency virus (HIV)-infected adults receiving antiretroviral therapy: Recommendations of the HIV Medical Association of the Infectious Disease Society of America and the Adult. Clin Infect Dis 2003;37:613–627 - PubMed
-
- Samaras K. The burden of diabetes and hyperlipidemia in treated HIV infection and approaches for cardiometabolic care. Curr HIV/AIDS Rep 2012;9:206–217 - PubMed
-
- Wohl DA, McComsey G, Tebas P, et al. Current concepts in the diagnosis and management of metabolic complications of HIV infection and its therapy. Clin Infect Dis 2006;43:645–653 - PubMed
-
- Boccara F, Lang S, Meuleman C, et al. HIV and coronary heart disease: Time for a better understanding. J Am Coll Cardiol 2013;61:511–523 - PubMed
-
- O'Halloran JA, Satchell CS, Mallon PWG. Dyslipidemia, atherosclerosis and cardiovascular disease: An increasingly important triad in an aging population living with HIV. Future Virol 2013;8:1021–1034
MeSH terms
Substances
Grants and funding
- R38 AI140299/AI/NIAID NIH HHS/United States
- U01 AI103397/AI/NIAID NIH HHS/United States
- U54 AG062334/AG/NIA NIH HHS/United States
- U01 AI031834/AI/NIAID NIH HHS/United States
- U01 AI034989/AI/NIAID NIH HHS/United States
- U01 AI034994/AI/NIAID NIH HHS/United States
- U01 AI103401/AI/NIAID NIH HHS/United States
- U01 AI103408/AI/NIAID NIH HHS/United States
- U01 HL146194/HL/NHLBI NIH HHS/United States
- U01 AI103390/AI/NIAID NIH HHS/United States
- U01 AI034993/AI/NIAID NIH HHS/United States
- U01 HL146203/HL/NHLBI NIH HHS/United States
- P30 AI050410/AI/NIAID NIH HHS/United States
- U01 AI042590/AI/NIAID NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
