

Estimating the fitness cost and benefit of cefixime resistance in Neisseria gonorrhoeae to inform prescription policy: A modelling study
- PMID: 29088226
- PMCID: PMC5663337
- DOI: 10.1371/journal.pmed.1002416
Estimating the fitness cost and benefit of cefixime resistance in Neisseria gonorrhoeae to inform prescription policy: A modelling study
Abstract
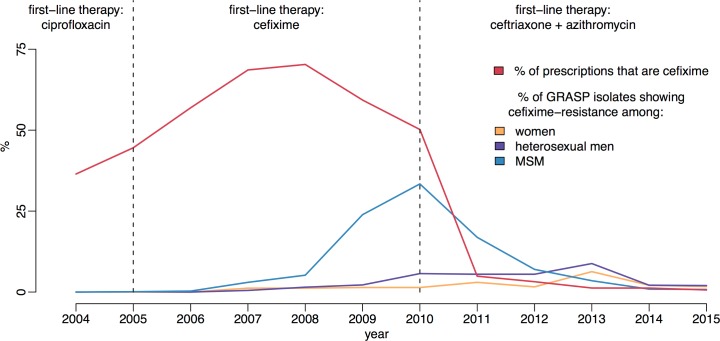
Background: Gonorrhoea is one of the most common bacterial sexually transmitted infections in England. Over 41,000 cases were recorded in 2015, more than half of which occurred in men who have sex with men (MSM). As the bacterium has developed resistance to each first-line antibiotic in turn, we need an improved understanding of fitness benefits and costs of antibiotic resistance to inform control policy and planning. Cefixime was recommended as a single-dose treatment for gonorrhoea from 2005 to 2010, during which time resistance increased, and subsequently declined.
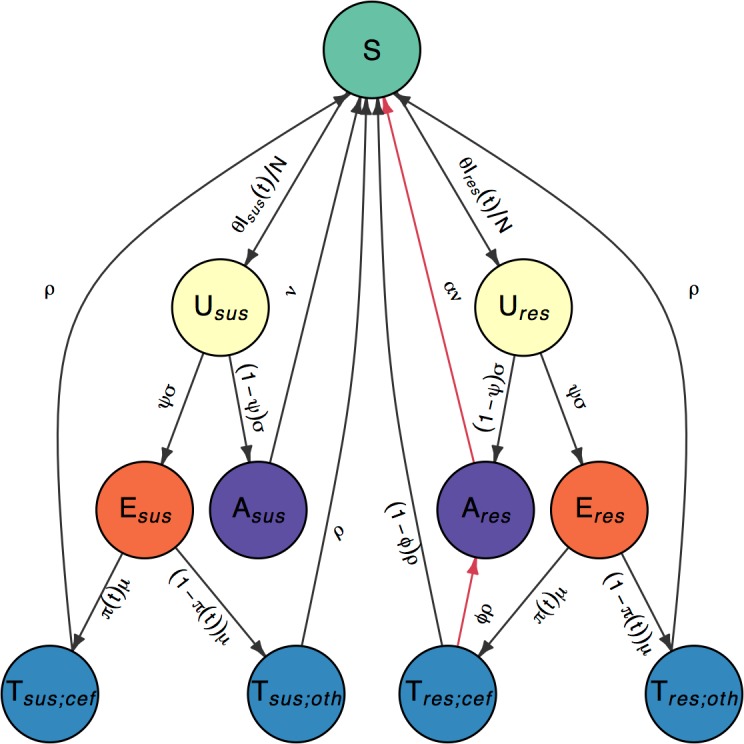
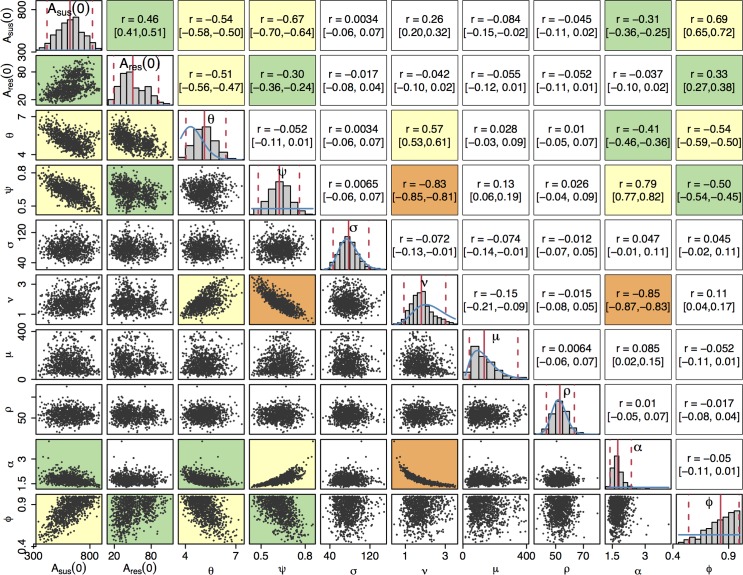
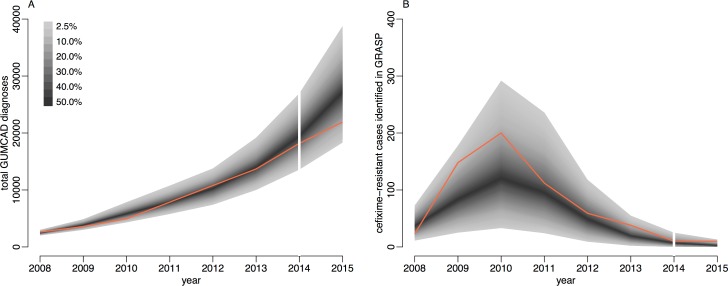
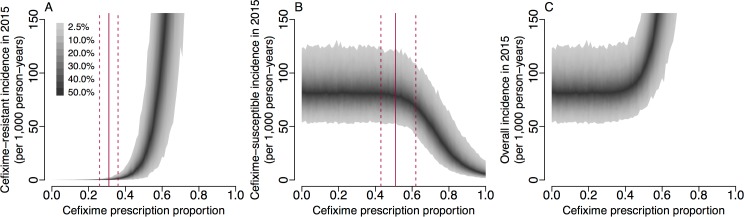
Methods and findings: We developed a stochastic compartmental model representing the natural history and transmission of cefixime-sensitive and cefixime-resistant strains of Neisseria gonorrhoeae in MSM in England, which was applied to data on diagnoses and prescriptions between 2008 and 2015. We estimated that asymptomatic carriers play a crucial role in overall transmission dynamics, with 37% (95% credible interval CrI 24%-52%) of infections remaining asymptomatic and untreated, accounting for 89% (95% CrI 82%-93%) of onward transmission. The fitness cost of cefixime resistance in the absence of cefixime usage was estimated to be such that the number of secondary infections caused by resistant strains is only about half as much as for the susceptible strains, which is insufficient to maintain persistence. However, we estimated that treatment of cefixime-resistant strains with cefixime was unsuccessful in 83% (95% CrI 53%-99%) of cases, representing a fitness benefit of resistance. This benefit was large enough to counterbalance the fitness cost when 31% (95% CrI 26%-36%) of cases were treated with cefixime, and when more than 55% (95% CrI 44%-66%) of cases were treated with cefixime, the resistant strain had a net fitness advantage over the susceptible strain. Limitations include sparse data leading to large intervals on key model parameters and necessary assumptions in the modelling of a complex epidemiological process.
Conclusions: Our study provides, to our knowledge, the first estimates of the fitness cost and benefit associated with resistance of the gonococcus to a clinically relevant antibiotic. Our findings have important implications for antibiotic stewardship and public health policies and, in particular, suggest that a previously abandoned antibiotic could be used again to treat a minority of gonorrhoea cases without raising resistance levels.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures

Comment in
-
Fitness cost and benefit of antimicrobial resistance in Neisseria gonorrhoeae: Multidisciplinary approaches are needed.PLoS Med. 2017 Oct 31;14(10):e1002423. doi: 10.1371/journal.pmed.1002423. eCollection 2017 Oct. PLoS Med. 2017. PMID: 29088232 Free PMC article.
References
-
- Public Health England. Infection Report: HIV—STIs. Public Health England; 2015. https://www.gov.uk/government/publications/health-protection-report-volu...
-
- Lewis DA. The Gonococcus fights back: is this time a knock out? Sexually Transmitted Infections. 2010;86(6):415–421. doi: 10.1136/sti.2010.042648 - DOI - PubMed
-
- Grad YH, Kirkcaldy RD, Trees D, Dordel J, Harris SR, Goldstein E, et al. Genomic epidemiology of Neisseria gonorrhoeae with reduced susceptibility to cefixime in the USA: A retrospective observational study. The Lancet Infectious Diseases. 2014;14(3):220–226. doi: 10.1016/S1473-3099(13)70693-5 - DOI - PMC - PubMed
-
- Bignell C, FitzGerald M. UK national guideline for the management of gonorrhoea in adults, 2011. International Journal of STD & AIDS. 2011;22(10):541–547. doi: 10.1258/ijsa.2011.011267 - DOI - PubMed
-
- Bignell C, Unemo M. 2012 European guideline on the diagnosis and treatment of gonorrhoea in adults. International Journal of STD & AIDS. 2013;24(2):85–92. doi: 10.1177/0956462412472837 - DOI - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
