

Out-of-pocket payment for surgery in Uganda: The rate of impoverishing and catastrophic expenditure at a government hospital
- PMID: 29088302
- PMCID: PMC5663485
- DOI: 10.1371/journal.pone.0187293
Out-of-pocket payment for surgery in Uganda: The rate of impoverishing and catastrophic expenditure at a government hospital
Abstract
Background and objectives: It is Ugandan governmental policy that all surgical care delivered at government hospitals in Uganda is to be provided to patients free of charge. In practice, however, frequent stock-outs and broken equipment require patients to pay for large portions of their care out of their own pocket. The purpose of this study was to determine the financial impact on patients who undergo surgery at a government hospital in Uganda.
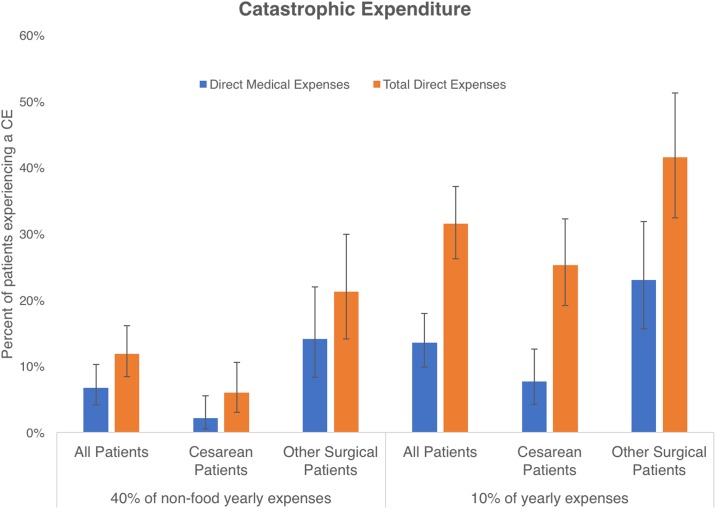
Methods: Every surgical patient discharged from a surgical ward at a large regional referral hospital in rural southwestern Uganda over a 3-week period in April 2016 was asked to participate. Patients who agreed were surveyed to determine their baseline level of poverty and to assess the financial impact of the hospitalization. Rates of impoverishment and catastrophic expenditure were then calculated. An "impoverishing expense" is defined as one that pushes a household below published poverty thresholds. A "catastrophic expense" was incurred if the patient spent more than 10% of their average annual expenditures.
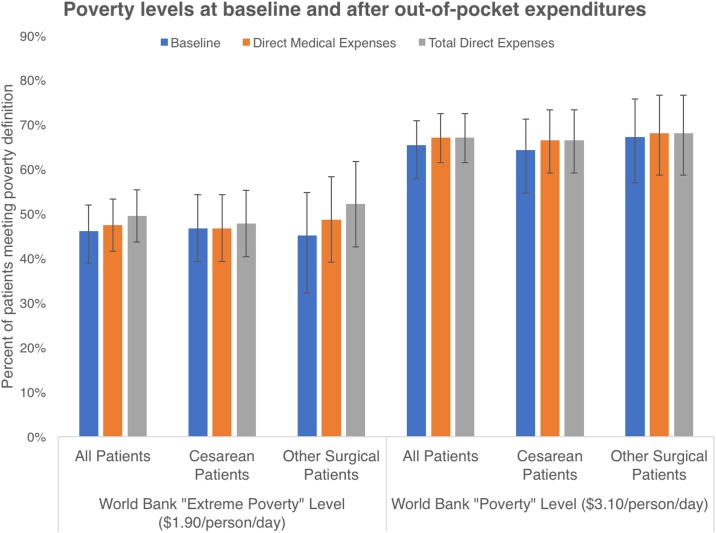
Results: We interviewed 295 out of a possible 320 patients during the study period. 46% (CI 40-52%) of our patients met the World Bank's definition of extreme poverty ($1.90/person/day). After receiving surgical care an additional 10 patients faced extreme poverty, and 5 patients were newly impoverished by the World Bank's definition ($3.10/person/day). 31% of patients faced a catastrophic expenditure of more than 10% of their estimated total yearly expenses. 53% of the households in our study had to borrow money to pay for care, 21% had to sell possessions, and 17% lost a job as a result of the patient's hospitalization. Only 5% of our patients received some form of charity.
Conclusions and relevance: Despite the government's policy to provide "free care," undergoing an operation at a government hospital in Uganda can result in a severe economic burden to patients and their families. Alternative financing schemes to provide financial protection are critically needed.
Conflict of interest statement
Figures
References
-
- Meara JG, Leather AJM, Hagander L, Alkire BC, Alonso N, Ameh EA, et al. Global Surgery 2030: evidence and solutions for achieving health, welfare, and economic development. The Lancet. 2015;386(9993):569–624. https://doi.org/10.1016/S0140-6736(15)60160-X. - DOI - PubMed
-
- Group TWB. World Bank Open Data: The World Bank Group; 2016 [updated Oct 17, 2017; cited 2016]. https://data.worldbank.org/.
-
- Rose J, Weiser TG, Hider P, Wilson L, Gruen RL, Bickler SW. Estimated need for surgery worldwide based on prevalence of diseases: a modelling strategy for the WHO Global Health Estimate. The Lancet Global Health. 2015;3(Supplement 2):S13–S20. https://doi.org/10.1016/S2214-109X(15)70087-2. - DOI - PMC - PubMed
-
- Weiser TG, Haynes AB, Molina G, Lipsitz SR, Esquivel MM, Uribe-Leitz T, et al. Size and distribution of the global volume of surgery in 2012. Bulletin of the World Health Organization. 2016;94(3):201–9F. doi: 10.2471/BLT.15.159293 - DOI - PMC - PubMed
-
- Chao TE, Sharma K, Mandigo M, Hagander L, Resch SC, Weiser TG, et al. Cost-effectiveness of surgery and its policy implications for global health: a systematic review and analysis. The Lancet Global Health. 2014;2(6):e334–e45. https://doi.org/10.1016/S2214-109X(14)70213-X. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
