

Effects of Co-occurring Genomic Alterations on Outcomes in Patients with KRAS-Mutant Non-Small Cell Lung Cancer
- PMID: 29089357
- PMCID: PMC5771996
- DOI: 10.1158/1078-0432.CCR-17-1841
Effects of Co-occurring Genomic Alterations on Outcomes in Patients with KRAS-Mutant Non-Small Cell Lung Cancer
Abstract
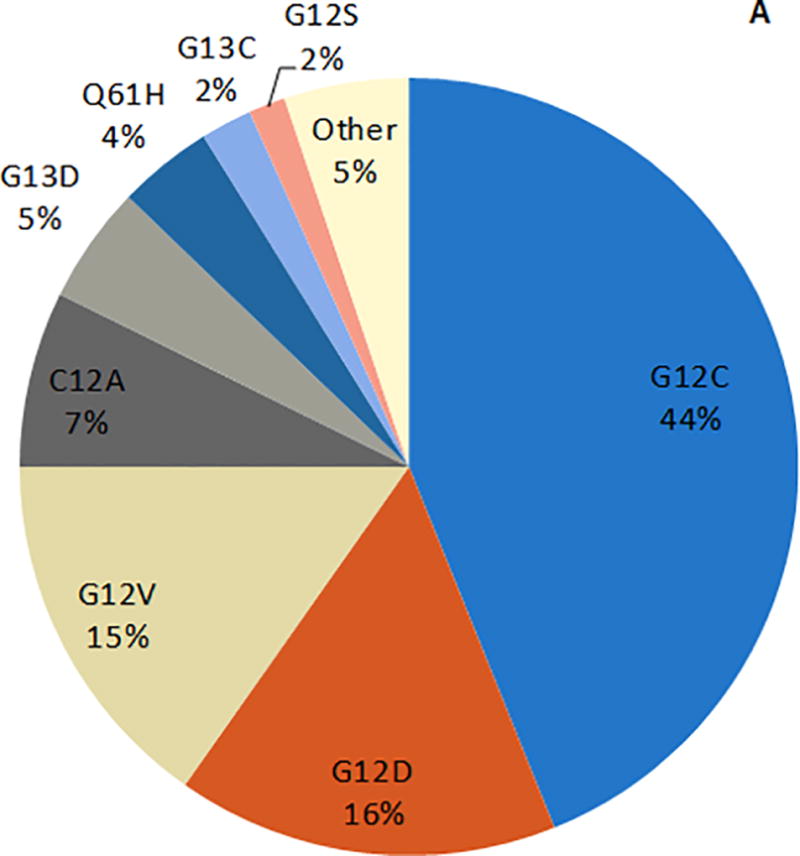
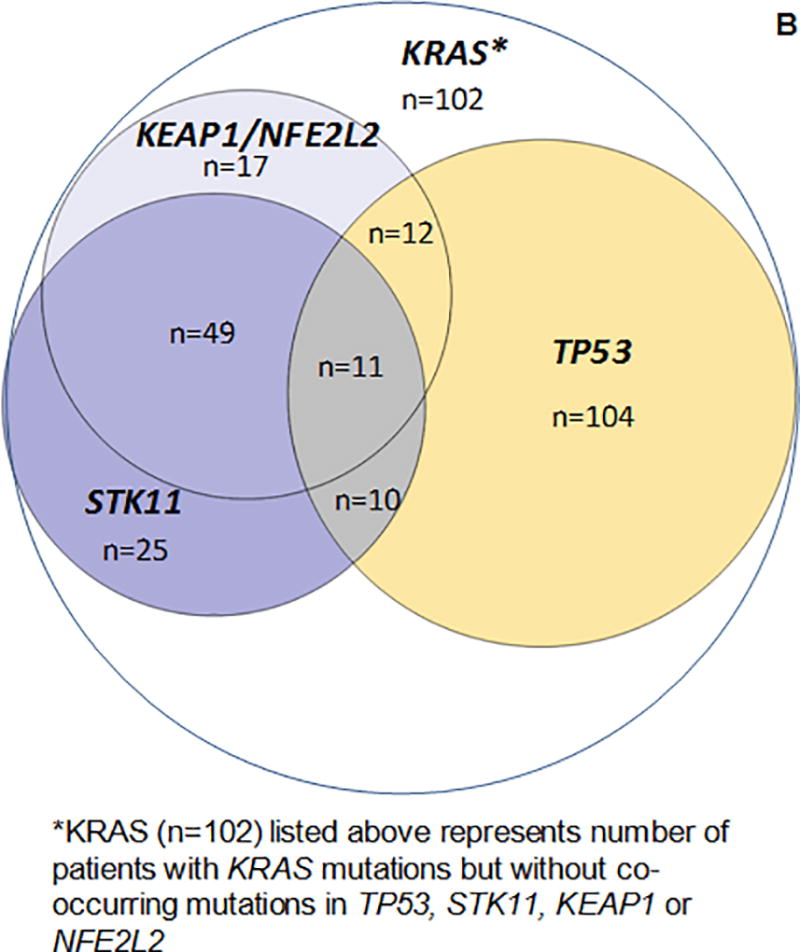
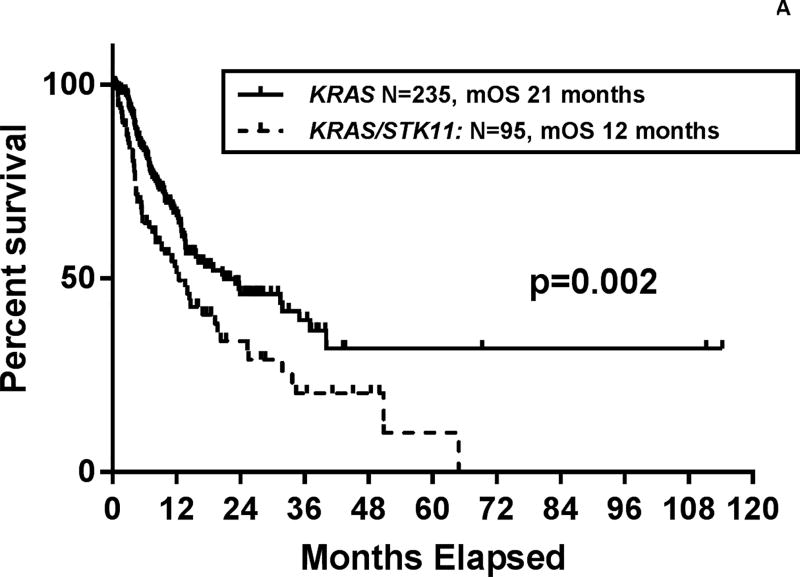
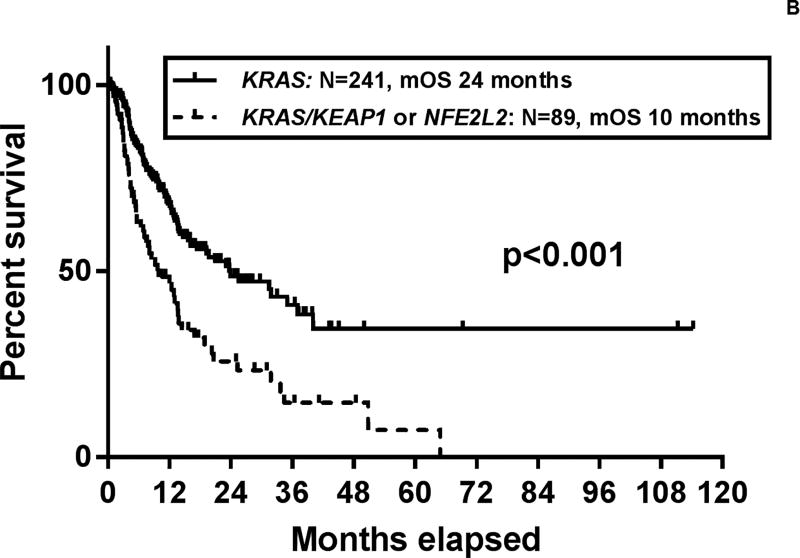
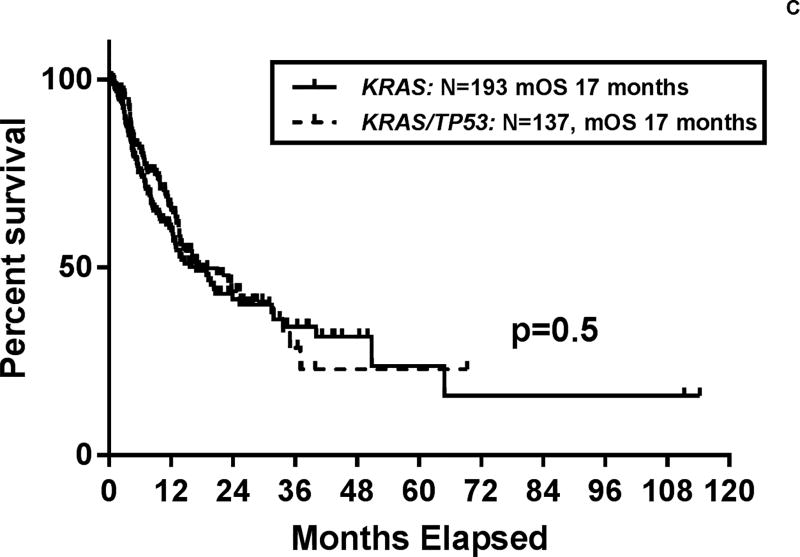
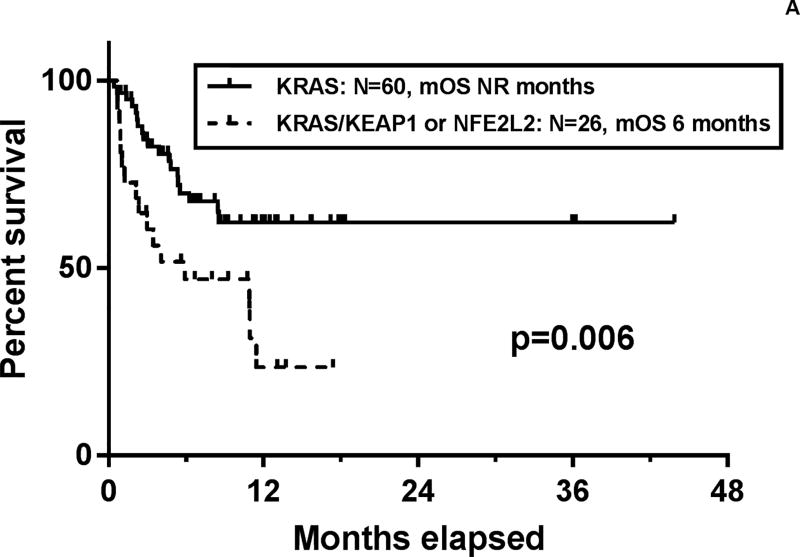
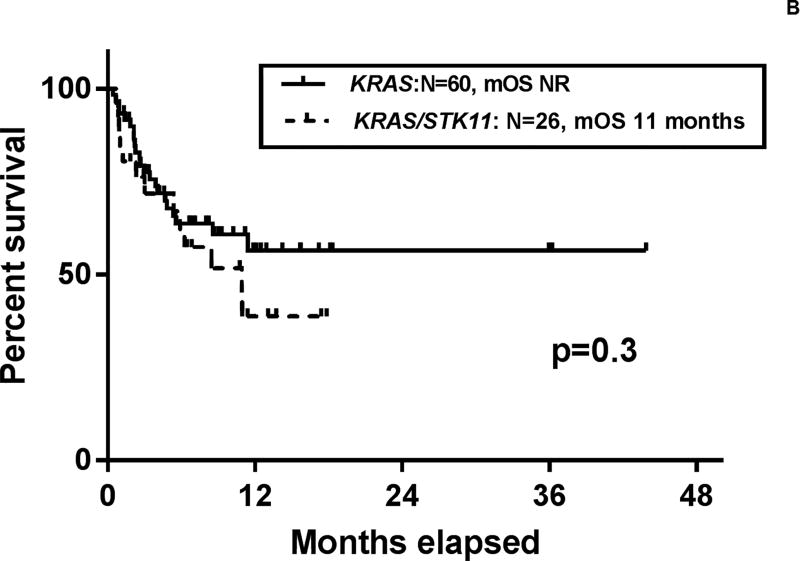
Purpose:KRAS mutations occur in approximately 25% of patients with non-small cell lung cancer (NSCLC). Despite the uniform presence of KRAS mutations, patients with KRAS-mutant NSCLC can have a heterogeneous clinical course. As the pattern of co-occurring mutations may describe different biological subsets of patients with KRAS-mutant lung adenocarcinoma, we explored the effects of co-occurring mutations on patient outcomes and response to therapy.Experimental Design: We identified patients with advanced KRAS-mutant NSCLC and evaluated the most common co-occurring genomic alterations. Multivariate analyses were performed incorporating the most frequent co-mutations and clinical characteristics to evaluate association with overall survival as well as response to platinum-pemetrexed chemotherapy and immune checkpoint inhibitors.Results: Among 330 patients with advanced KRAS-mutant lung cancers, the most frequent co-mutations were found in TP53 (42%), STK11 (29%), and KEAP1/NFE2L2 (27%). In a multivariate analysis, there was a significantly shorter survival in patients with co-mutations in KEAP1/NFE2L2 [HR, 1.96; 95% confidence interval (CI), 1.33-2.92; P ≤ 0.001]. STK11 (HR, 1.3; P = 0.22) and TP53 (HR 1.11, P = 0.58) co-mutation statuses were not associated with survival. Co-mutation in KEAP1/NFE2L2 was also associated with shorter duration of initial chemotherapy (HR, 1.64; 95% CI, 1.04-2.59; P = 0.03) and shorter overall survival from initiation of immune therapy (HR, 3.54; 95% CI, 1.55-8.11; P = 0.003).Conclusions: Among people with KRAS-mutant advanced NSCLC, TP53, STK11, and KEAP1/NFE2L2 are the most commonly co-occurring somatic genomic alterations. Co-mutation of KRAS and KEAP1/ NFE2L2 is an independent prognostic factor, predicting shorter survival, duration of response to initial platinum-based chemotherapy, and survival from the start of immune therapy. Clin Cancer Res; 24(2); 334-40. ©2017 AACR.
©2017 American Association for Cancer Research.
Figures
Comment in
-
It's far better to be alone than to be in bad company.J Thorac Dis. 2019 Mar;11(3):649-651. doi: 10.21037/jtd.2019.02.65. J Thorac Dis. 2019. PMID: 31019750 Free PMC article. No abstract available.
References
-
- Linardou H, Dahabreh IJ, Kanaloupiti D, et al. Assessment of somatic k-RAS mutations as a mechanism associated with resistance to EGFR-targeted agents: a systematic review and meta-analysis of studies in advanced non-small-cell lung cancer and metastatic colorectal cancer. Lancet Oncol. 2008;9(10):962–972. doi: 10.1016/S1470-2045(08)70206-7. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
