

The Pros and Cons of Computer-Aided Surgery for Segmental Mandibular Reconstruction after Oncological Surgery
- PMID: 29090194
- PMCID: PMC5647851
- DOI: 10.7181/acfs.2017.18.3.149
The Pros and Cons of Computer-Aided Surgery for Segmental Mandibular Reconstruction after Oncological Surgery
Abstract
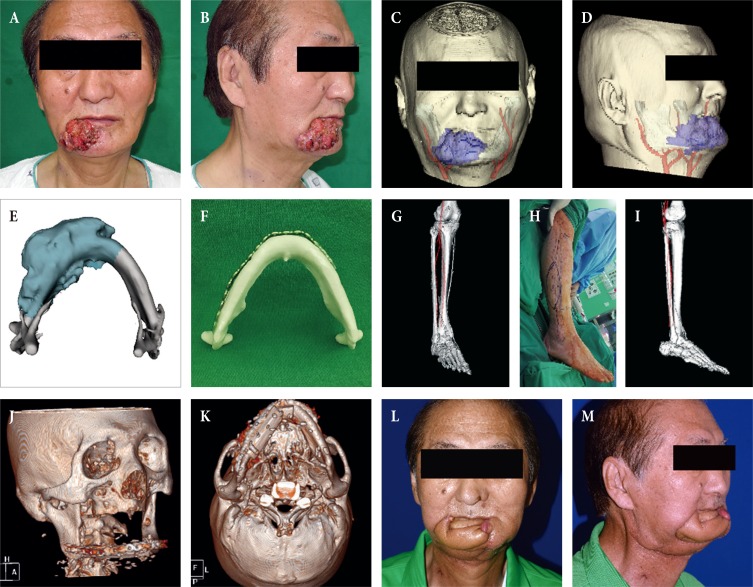
Computer-aided surgery (CAS) started being used for head and neck reconstruction in the late 2000s. Its use represented a paradigm shift, changing the concept of head and neck reconstruction as well as mandible reconstruction. Reconstruction using CAS proceeds through 4 phases: planning, modeling, surgery, and evaluation. Thus, it can overcome a number of trial-and-error issues which may occur in the operative field and reduce surgical time. However, if it is used for oncologic surgery, it is difficult to evaluate tumor margins during tumor surgery, thereby restricting pre-surgical planning. Therefore, it is dangerous to predetermine the resection margins during the pre-surgical phase and the variability of the resection margins must be taken into consideration. However, it allows for the preparation of a prebending plate and planning of an osteotomy site before an operation, which are of great help. If the current problems are resolved, its applications can be greatly extended.
Keywords: Computer-aided surgery; Mandible; Mandibular reconstruction; Microsurgical free flaps; Resection margin.
Conflict of interest statement
No potential conflict of interest relevant to this article was reported.
Figures
References
-
- Hou JS, Chen M, Pan CB, Tao Q, Wang JG, Wang C, et al. Immediate reconstruction of bilateral mandible defects: management based on computer-aided design/computer-aided manufacturing rapid prototyping technology in combination with vascularized fibular osteomyocutaneous flap. J Oral Maxillofac Surg. 2011;69:1792–1797. - PubMed
-
- Hayden RE, Mullin DP, Patel AK. Reconstruction of the segmental mandibular defect: current state of the art. Curr Opin Otolaryngol Head Neck Surg. 2012;20:231–236. - PubMed
-
- Cordeiro PG, Disa JJ, Hidalgo DA, Hu QY. Reconstruction of the mandible with osseous free flaps: a 10-year experience with 150 consecutive patients. Plast Reconstr Surg. 1999;104:1314–1320. - PubMed
-
- Hidalgo DA, Pusic AL. Free-flap mandibular reconstruction: a 10-year follow-up study. Plast Reconstr Surg. 2002;110:438–449. - PubMed
-
- He Y, Zhang ZY, Zhu HG, Sader R, He J, Kovacs AF. Free fibula osteocutaneous flap for primary reconstruction of T3-T4 gingival carcinoma. J Craniofac Surg. 2010;21:301–305. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
