

Postoperative analgesic efficiency of transversus abdominis plane block after ventral hernia repair: a prospective, randomized, controlled clinical trial
- PMID: 29090265
- PMCID: PMC5642852
- DOI: 10.21454/rjaic.7518.242.chv
Postoperative analgesic efficiency of transversus abdominis plane block after ventral hernia repair: a prospective, randomized, controlled clinical trial
Abstract
Background and aims: Effective postoperative analgesia is a key element in reducing postoperative morbidity, accelerating recovery and avoiding chronic postoperative pain. The aim of this study was to evaluate the effectiveness of ultrasound-guided Transversus Abdominis Plane (TAP) block, performed before surgical incision, in providing postoperative analgesia for patients undergoing open ventral hernia repair under general anaesthesia.
Methods: Seventy elective patients scheduled for open ventral hernia repair surgery under general anaesthesia were divided randomly into two equal groups: Group I received bilateral TAP block performed before surgical incision (n = 35); Group II received systemic postoperative analgesia with parenteral opioid (morphine) alone (n = 35). Postoperatively pain scores at rest and with movement, total morphine consumption and opioid related side effects were recorded.
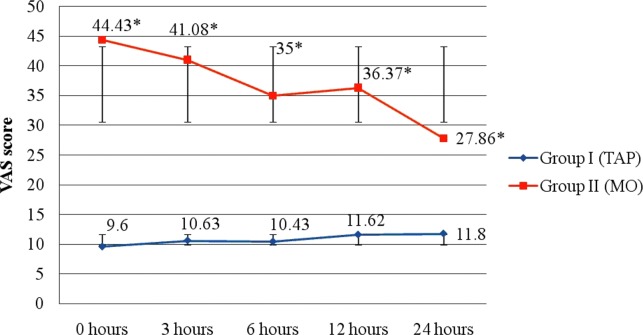
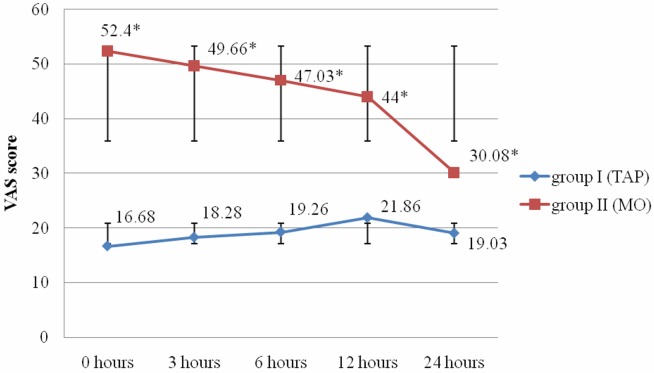
Results: Postoperative pain scores at rest and mobilization/cough were significantly higher in patients without TAP block (p < 0.05). Mean intraoperative fentanyl consumption was comparable between the two groups: 0.75 ± 0.31 mg in group I (TAP) and 0.86 ± 0.29 mg in group II (MO), p = 0.1299. Patients undergoing preincisional TAP block had reduced morphine requirements during the first 24 hours after surgery, compared to patients from group II, without TAP block (p = 0.0001). There was no difference in the incidence of opioid related side effects (nausea, vomiting) in the both groups during the first 24 postoperative hours.
Conclusion: The use of preincisional ultrasound guided TAP block reduced the pain scores at rest and with movement/cough, opioid consumption and opioid-related side effects after ventral hernia repair when compared with opioid-only analgesia.
Keywords: pain management; postoperative pain; transversus abdominis plane block; ventral hernia.
Conflict of interest statement
Conflict of interest Nothing to declare
Figures
References
-
- Wickström K. Postoperative pain management – predictors, barriers and outcome. Göteborg: Sahlgrenska Academy; 2008.
-
- Moizo E, Berti M, Marchetti C, Deni F, Albertin A, Muzzolon F, et al. Acute Pain Service and multimodal therapy for postsurgical pain control: evaluation of protocol efficacy. Minerva Anestesiol. 2004;70:779–787. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
Miscellaneous