

Are there synergies from combining hygiene and sanitation promotion campaigns: Evidence from a large-scale cluster-randomized trial in rural Tanzania
- PMID: 29091726
- PMCID: PMC5665426
- DOI: 10.1371/journal.pone.0186228
Are there synergies from combining hygiene and sanitation promotion campaigns: Evidence from a large-scale cluster-randomized trial in rural Tanzania
Abstract
Summary: The current evidence on handwashing and sanitation programs suggests limited impacts on health when at-scale interventions have been tested in isolation. However, no published experimental evidence currently exists that tests the interaction effects between sanitation and handwashing. We present the results of two large-scale, government-led handwashing and sanitation promotion campaigns in rural Tanzania, with the objective of tracing the causal chain from hygiene and sanitation promotion to changes in child health outcomes and specifically testing for potential interaction effects of combining handwashing and sanitation interventions.
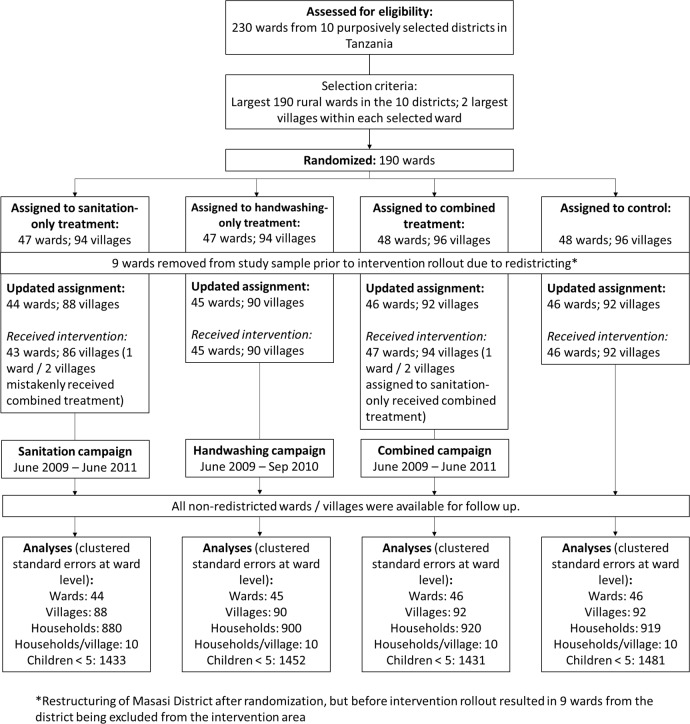
Methods: The study is a factorial cluster-randomized control trial where 181 rural wards from 10 districts in Tanzania were randomly assigned to receive sanitation promotion, handwashing promotion, both interventions together or neither (control). Interventions were rolled out from February 2009 to June 2011 and the endline survey was conducted from May to November 2012, approximately one year after program completion. The sample was composed of households with children under 5 years old in the two largest villages in each ward. Masking was not possible due to the nature of the intervention, but enumerators played no part in the intervention and were blinded to treatment status. The primary outcome of interest was 7-day diarrhea prevalence for children under five. Intermediate outcomes of behavior change including improved latrine construction, levels of open defecation and handwashing with soap were also analyzed. Secondary health outcomes included anemia, height-for-age and weight-for-age of children under 5. An intention-to-treat analysis was used to assess the relationship between the interventions and outcomes of interest.
Findings: One year after the end of the program, ownership of improved latrines increased from 49.7% to 64.8% (95% CI 57.9%-71.7%) and regular open defecation decreased from 23.1% to 11.1% (95% CI 3.5%-18.7%) in sanitation promotion-only wards. Households in handwashing promotion-only wards showed marginal improvements in handwashing behavior related to food preparation but not at other critical junctures. There were no detectable interaction effects for the combined intervention. The associated cost-per-household gaining access to improved sanitation is estimated to be USD $194. Final effects on child health measured through diarrhea, anemia, stunting and wasting were absent in all treatment groups.
Interpretation: Although statistically significant, the changes in intermediate outcomes achieved through each intervention in isolation were not large enough to generate meaningful health impacts. With no observable signs of interaction, the combined intervention produced similar results. The study highlights the importance of focusing on intermediate outcomes of take up and behavior change as a critical first step in large-scale programs before realizing the changes in health that sanitation and hygiene interventions aim to deliver.
Trial registration: Clinicaltrials.gov NCT01465204.
Conflict of interest statement
Figures
References
-
- WHO-Unicef. Levels and Trends in Child Mortality. Report 2013. World Health Organization
-
- Humphrey JH. Child undernutrition, tropical enteropathy, toilets, and handwashing. The Lancet. 2009. September 19;374(9694):1032–5. - PubMed
-
- Chase C, Do QT. Handwashing behavior change at scale: evidence from a randomized evaluation in Vietnam. World Bank Policy Research Working Paper. 2012 Sep 1(6207).
-
- Galiani S, Gertler P, Ajzenman N, Orsola‐Vidal A. Promoting Handwashing Behavior: The Effects of Large‐scale Community and School‐level Interventions. Health economics. 2015. January 1. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
