

The Renoprotective Effects of Docosahexaenoic Acid as an Add-on Therapy in Patients Receiving Eicosapentaenoic Acid as Treatment for IgA Nephropathy: A Pilot Uncontrolled Trial
- PMID: 29093399
- PMCID: PMC5820033
- DOI: 10.2169/internalmedicine.9155-17
The Renoprotective Effects of Docosahexaenoic Acid as an Add-on Therapy in Patients Receiving Eicosapentaenoic Acid as Treatment for IgA Nephropathy: A Pilot Uncontrolled Trial
Abstract
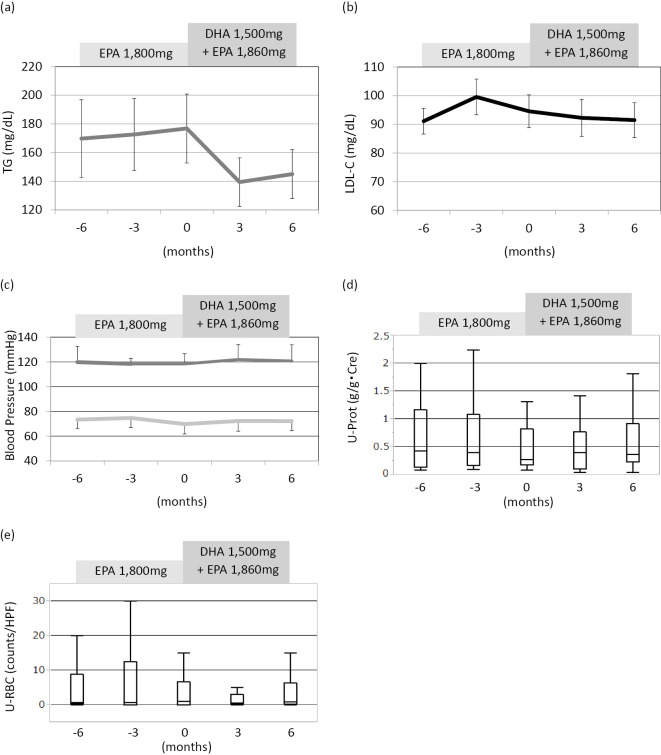
Objective Docosahexaenoic acid (DHA) and eicosapentaenoic acid (EPA) have been reported to have beneficial effects in patients with IgA nephropathy (IgAN). Although DHA and EPA have different mechanisms of action, no study to date has assessed their individual actions in patients with IgAN. This study therefore analyzed the effects administering DHA in addition to EPA for the treatment of IgAN. Methods Twenty-one IgAN patients who were being treated with EPA (1,800 mg/day) were switched to EPA (1,860 mg/day) and DHA (1,500 mg/day). The changes in their clinical parameters from 6 months before to 6 months after switching treatment were analyzed. Results The triglyceride levels did not change during treatment with EPA alone, but tended to decrease-although not to a statistically significant extent-after the switch. The patients' low-density-lipoprotein cholesterol, blood pressure, proteinuria, and hematuria levels were similar before and after switching. The estimated glomerular filtration rate (eGFR) tended to decrease during EPA therapy, but became stable after switching and the median %⊿eGFR changed from -7.354% during EPA therapy to +1.26% during the 6 months after switching to EPA and DHA therapy (p=0.00132), and renal the function remained stable for another 6 months. Moreover, the median %⊿eGFR during the 6 months after switching was significantly higher in comparison to IgAN patients who were treated with EPA alone as a control (-3.26%, p=0.0361). No clinical parameters were independently associated with a stable renal function without switching to DHA/EPA. Conclusion The addition of DHA to EPA stabilized the renal function of IgAN patients, and it seemed that there were pleiotropic effects beyond the improvement of the clinical parameters.
Keywords: IgA nephropathy; docosahexaenoic acid; eicosapentaenoic acid; fish oil; omega-3 polyunsaturated acid.
Figures

References
-
- Berger J, Hinglais N. Intercapillary deposits of IgA-IgG. J Urol Nephrol 74: 694-695, 1968. - PubMed
-
- Komatsu H, Fujimoto S, Hara S, et al. Recent therapeutic strategies improve renal outcome in patients with IgA nephropathy. Am J Nephrol 30: 19-25, 2009. - PubMed
-
- Philip CC, Purveen Y. Omega-3 polyunsaturated fatty acids and human health outcomes. Biofactors 35: 266-372, 2009. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous