

Predictors of survival and ability to wean from short-term mechanical circulatory support device following acute myocardial infarction complicated by cardiogenic shock
- PMID: 29094607
- PMCID: PMC6911658
- DOI: 10.1177/2048872617740834
Predictors of survival and ability to wean from short-term mechanical circulatory support device following acute myocardial infarction complicated by cardiogenic shock
Abstract
Background:: Cardiogenic shock following acute myocardial infarction (AMI-CS) portends a poor prognosis. Short-term mechanical circulatory support devices (MCSDs) provide hemodynamic support for patients with cardiogenic shock but predictors of survival and the ability to wean from short-term MCSDs remain largely unknown.
Methods:: All patients > 18 years old treated at our institution with extra-corporeal membrane oxygenation or short-term surgical ventricular assist device for AMI-CS were studied. We collected acute myocardial infarction details with demographic and hemodynamic variables. Primary outcomes were survival to discharge and recovery from MCSD (i.e. survival without heart replacement therapy including durable ventricular assist device or heart transplant).
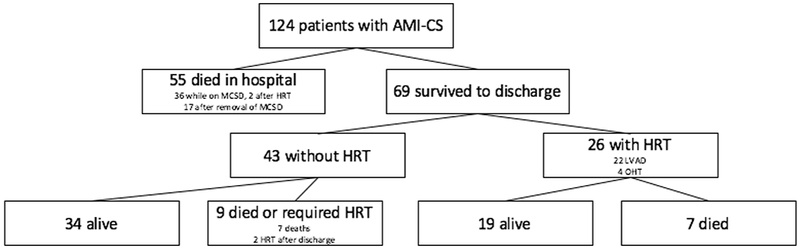
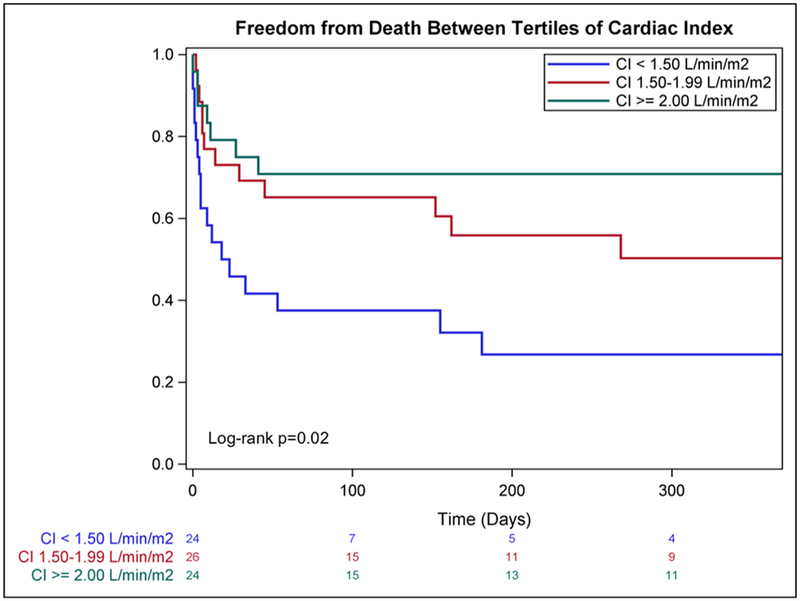
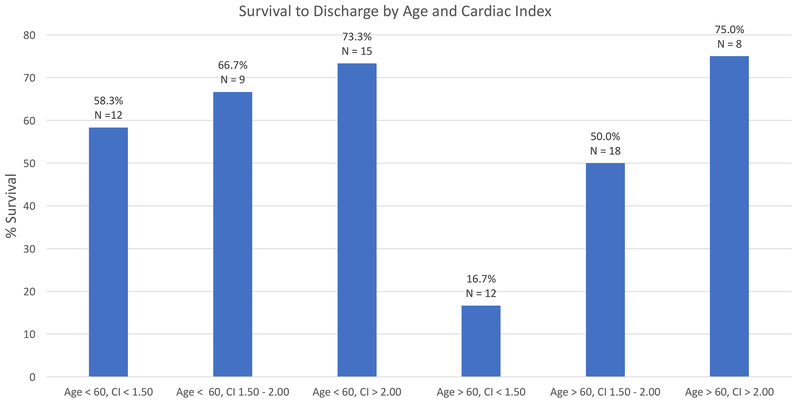
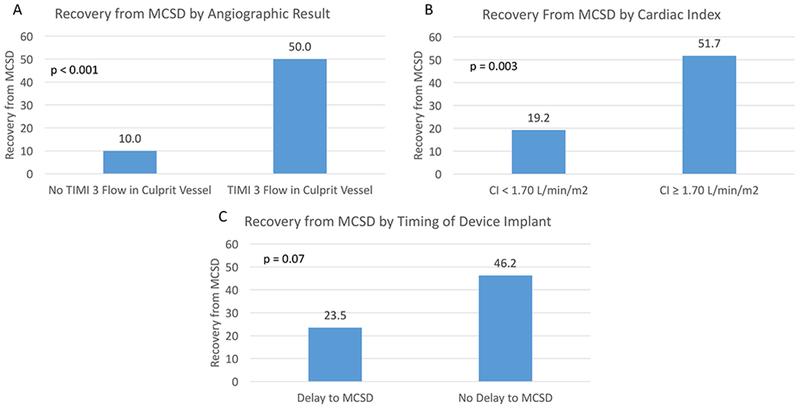
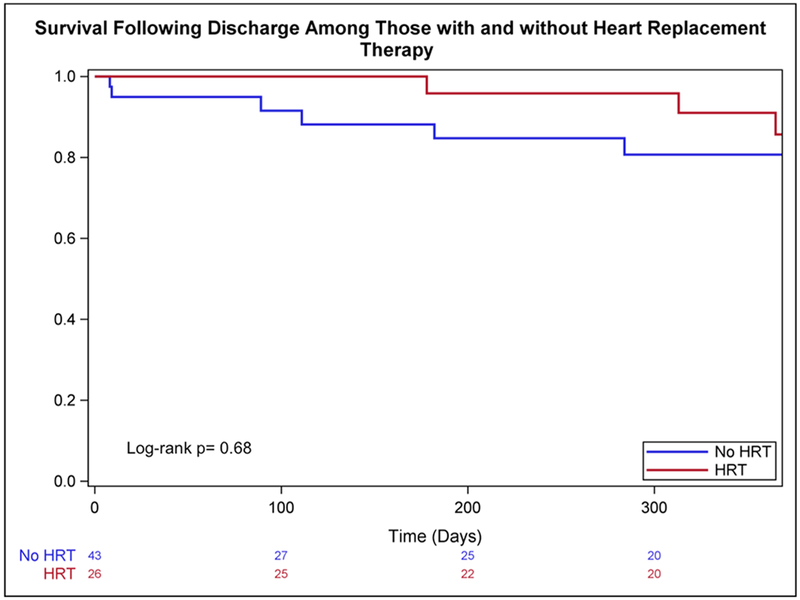
Results:: One hundred and twenty-four patients received extra-corporeal membrane oxygenation or short-term surgical ventricular assist device following acute myocardial infarction from 2007 to 2016; 89 received extra-corporeal membrane oxygenation and 35 short-term ventricular assist device. Fifty-five (44.4%) died in the hospital and 69 (55.6%) survived to discharge. Twenty-six (37.7%) required heart replacement therapy (four transplant, 22 durable ventricular assist device) and 43 (62.3%) were discharged without heart replacement therapy. Age and cardiac index at MCSD implantation were predictors of survival to discharge; patients over 60 years with cardiac index <1.5 l/min per m2 had a low likelihood of survival. The angiographic result after revascularization predicted recovery from MCSD (odds ratio 9.00, 95% confidence interval 2.45-32.99, p=0.001), but 50% of those optimally revascularized still required heart replacement therapy. Cardiac index predicted recovery from MCSD among this group (odds ratio 4.06, 95% confidence interval 1.45-11.55, p=0.009).
Conclusion:: Among AMI-CS patients requiring short-term MCSDs, age and cardiac index predict survival to discharge. Angiographic result and cardiac index predict ventricular recovery but 50% of those optimally revascularized still required heart replacement therapy.
Keywords: ECMO; Myocardial infarction; cardiogenic shock; mechanical circulatory support; recovery; ventricular assist device.
Figures
References
-
- Goldberg RJ, Makam RC, Yarzebski J, McManus DD, Lessard D, Gore JM. Decade-Long Trends (2001-2011) in the Incidence and Hospital Death Rates Associated with the In-Hospital Development of Cardiogenic Shock after Acute Myocardial Infarction. Circ Cardiovasc Qual Outcomes. 2016;9:117–25. - PMC - PubMed
-
- Stretch R, Sauer CM, Yuh DD, Bonde P. National trends in the utilization of short-term mechanical circulatory support: incidence, outcomes, and cost analysis. J Am Coll Cardiol. 2014;64:1407–15. - PubMed
-
- Ouweneel DM, Eriksen E, Sjauw KD, et al. Percutaneous Mechanical Circulatory Support Versus Intra-Aortic Balloon Pump in Cardiogenic Shock After Acute Myocardial Infarction. J Am Coll Cardiol. 2017;69:278–287. - PubMed
-
- Takayama H, Truby L, Koekort M, et al. Clinical outcome of mechanical circulatory support for refractory cardiogenic shock in the current era. J Heart Lung Transplant. 2013;32:106–11. - PubMed
-
- Hochman JS, Sleeper LA, Webb JG, et al. Early revascularization in acute myocardial infarction complicated by cardiogenic shock. SHOCK Investigators. Should We Emergently Revascularize Occluded Coronaries for Cardiogenic Shock. N Engl J Med. 1999;341:625–34. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
