

Percutaneous transhepatic gallbladder drainage followed by elective laparoscopic cholecystectomy for patients with moderate to severe acute cholecystitis
- PMID: 29095318
- PMCID: PMC5682837
- DOI: 10.1097/MD.0000000000008533
Percutaneous transhepatic gallbladder drainage followed by elective laparoscopic cholecystectomy for patients with moderate to severe acute cholecystitis
Abstract
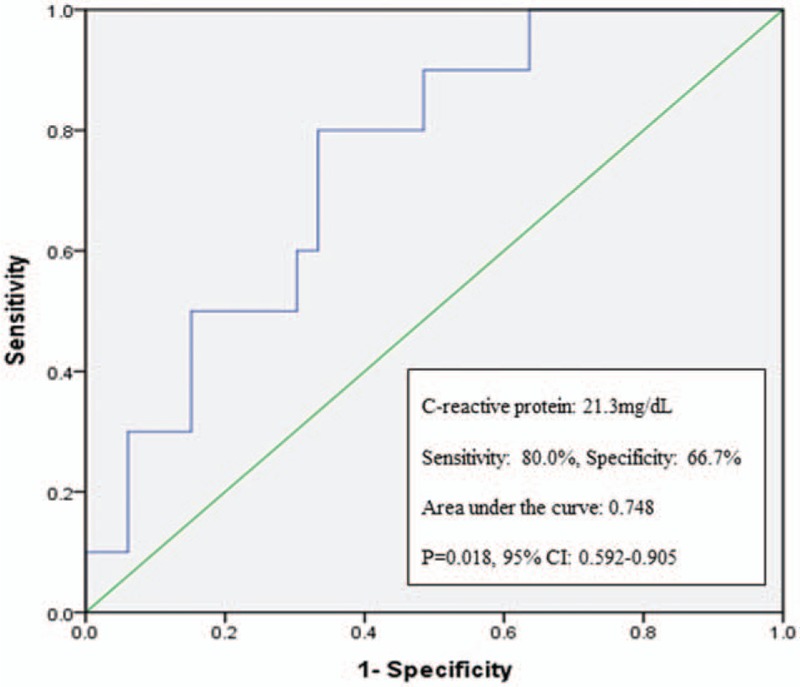
Percutaneous transhepatic gallbladder drainage followed by laparoscopic cholecystectomy (PTGBD+LC) is one treatment option for patients with moderate to severe acute cholecystitis (AC). However, the impact of PTGBD on operative difficulties in performing LC is controversial. We designed this retrospective study to clarify the surgical outcomes after PTGBD+LC for the management of patients with moderate to severe AC.The medical records of 85 patients who underwent LC for moderate to severe AC from January 2013 to September 2016 were evaluated. They were divided into 2 groups based on the type of management: group A received PTGBD+LC, and group B received LC without drainage. We compared the patient characteristics, laboratory data which were obtained immediately before surgery or PTGBD at index admission, and surgical outcomes between the 2 groups. We also evaluated possible predictive factors associated with prolonged operative duration after PTGBD+LC.Patients in group A were older and had more comorbidities than those in group B. The laboratory tests obtained at index admission in group A showed higher serum levels of C-reactive protein (CRP) and alkaline phosphatase, and lower albumin levels than those in group B. The surgical outcomes after LC were similar between the 2 groups. However, operative duration was significantly shorter in group A (P = .012). In group A, a higher serum level of CRP was a predictive factor for a prolonged operation (hazard ratio 1.126; 95% confidence interval 1.012-1.253; P = .029). In conclusion, PTGBD+LC can shorten the operative duration in patients with moderate to severe AC, which might improve surgical outcomes in elderly patients with comorbidities, and elevated CRP values predicted a prolonged operation after PTGBD.
Conflict of interest statement
The authors declare conflict of interest.
Figures
References
-
- Overby DW, Apelgren KN, Richardson W, et al. SAGES guidelines for the clinical application of laparoscopic biliary tract surgery. Surg Endosc 2010;24:2368–86. - PubMed
-
- Radder RW. Ultrasonically guided percutaneous catheter drainage for gallbladder empyema. Diagn Imaging 1980;49:330–3. - PubMed
-
- Miura F, Takada T, Strasberg SM, et al. TG13 flowchart for the management of acute cholangitis and cholecystitis. J Hepatobiliary Pancreat Sci 2013;20:47–54. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
