

Malignant pheochromocytoma with multiple vertebral metastases causing acute incomplete paralysis during pregnancy: Literature review with one case report
- PMID: 29095319
- PMCID: PMC5682838
- DOI: 10.1097/MD.0000000000008535
Malignant pheochromocytoma with multiple vertebral metastases causing acute incomplete paralysis during pregnancy: Literature review with one case report
Abstract
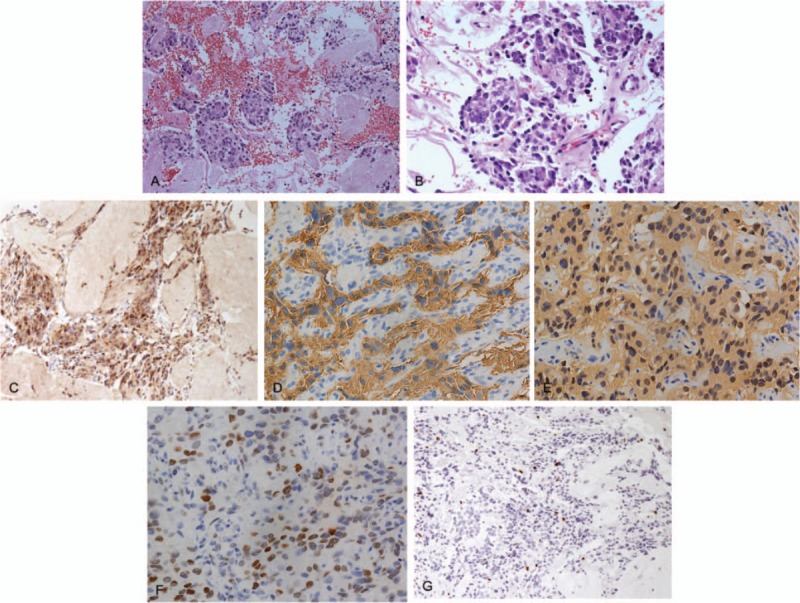
Rationale: We present a rare case of malignant pheochromocytoma with thoracic metastases during pregnancy that presented with symptoms of myelopathy and was treated with circumferential decompression, stabilization, and radiation. The management of this unique case is not well documented. The clinical manifestations, imaging results, pathological characteristics, treatment and prognosis of the case were analyzed.
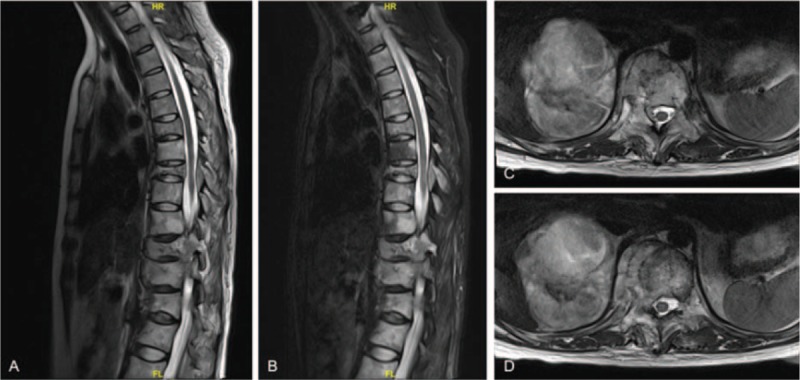
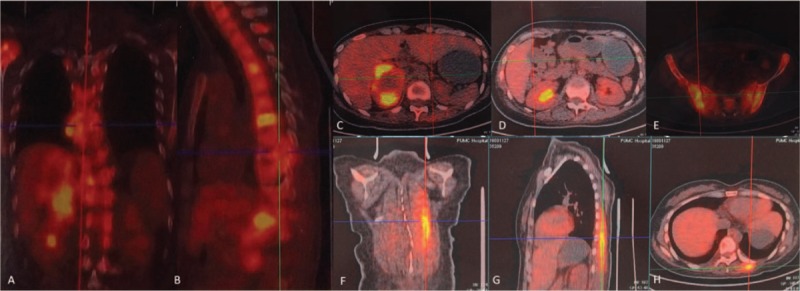
Patient concerns: A 26-year-old pregnant woman with a history of paroxysmal hypertension during the second trimester presented with lower extremity weakness, numbness, urinary incontinence, and back pain. Imaging studies revealed a right adrenal pheochromocytoma, multiple metastases at T8, T11, T12, and the pelvis girdle causing significant multilevel cord compression and significant osteolytic lesions at T11 and T12.
Diagnoses: We believe this is the first reported case of metastatic pheochromocytoma of the thoracic spine presenting with symptoms of myelopathy during pregnancy.
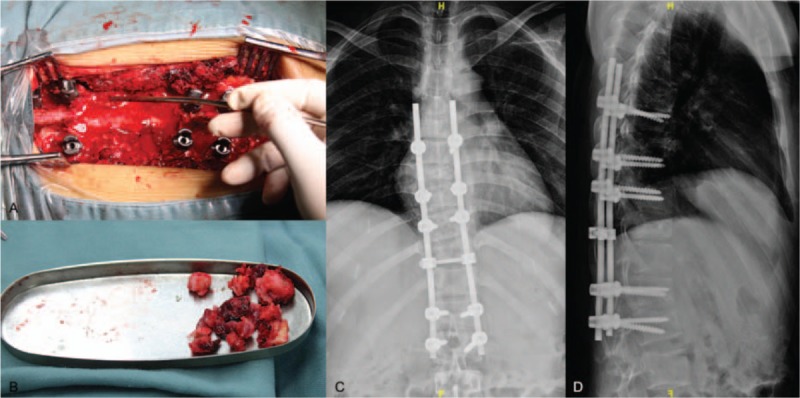
Interventions: A healthy neonate was delivered by emergency caesarean section at 34 weeks. Subsequently, the patient underwent a circumferential spinal cord decompression and a stabilization procedure.
Outcomes: The patient's neurological deficits improved significantly after the surgery, and the postoperative period was uneventful at the 6-month follow-up visit.
Lessons: This article emphasizes that metastatic pheochromocytoma of the spine, although rare, should be part of the differential when a patient presents with elevated blood pressure, weakness, and urinary incontinence.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures
References
-
- Kaloostian PE, Zadnik PL, Kim JE, et al. High incidence of morbidity following resection of metastatic pheochromocytoma in the spine. J Neurosurg Spine 2014;20:726–33. - PubMed
-
- Kaloostian PE, Zadnik PL, Awad AJ, et al. En bloc resection of a pheochromocytoma metastatic to the spine for local tumor control and for treatment of chronic catecholamine release and related hypertension. J Neurosurg Spine 2013;18:611–6. - PubMed
-
- Kheir E, Pal D, Mohanlal P, et al. Cervical spine metastasis from adrenal pheochromocytoma. Acta Neurochir (Wien) 2006;148:1219–20. - PubMed
-
- Mori S, Okura T, Kitami Y, et al. A case of metastatic extra-adrenal pheochromocytoma 12 years after surgery. Hypertens Res 2002;25:141–4. - PubMed
-
- Yurt A, Arda MN, Vardar E. Metastatic pheochromocytoma of the thoracic spinal extradural space. Case report and review of the literature. Kobe J Med Sci 2005;51:49–53. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
