

Accuracy of a screening tool for medication adherence: A systematic review and meta-analysis of the Morisky Medication Adherence Scale-8
- PMID: 29095870
- PMCID: PMC5667769
- DOI: 10.1371/journal.pone.0187139
Accuracy of a screening tool for medication adherence: A systematic review and meta-analysis of the Morisky Medication Adherence Scale-8
Erratum in
-
Correction: Accuracy of a screening tool for medication adherence: A systematic review and meta-analysis of the Morisky Medication Adherence Scale-8.PLoS One. 2018 Apr 17;13(4):e0196138. doi: 10.1371/journal.pone.0196138. eCollection 2018. PLoS One. 2018. PMID: 29664949 Free PMC article.
Abstract
Background: This systematic review examined the reliability and validity of the Morisky Medication Adherence Scale-8 (MMAS-8), which has been widely used to assess patient medication adherence in clinical research and medical practice.
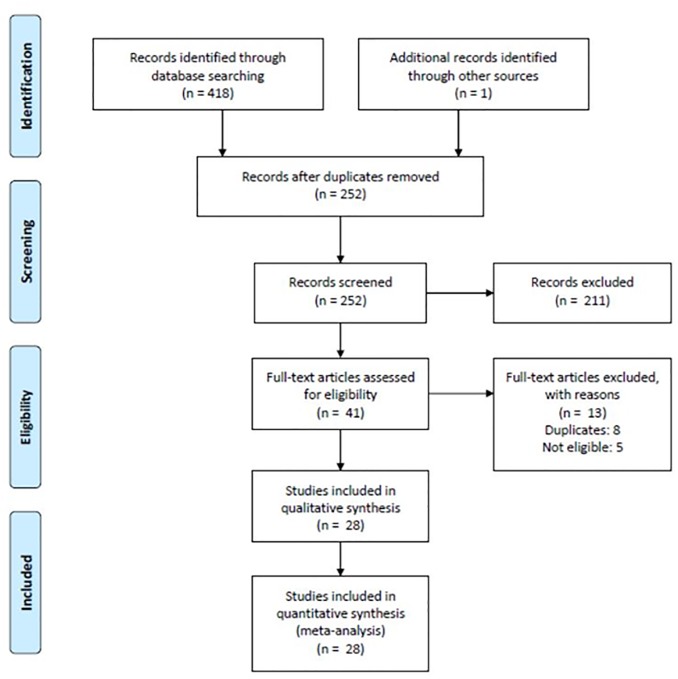
Methods: Of 418 studies identified through searching 4 electronic databases, we finally analyzed 28 studies meeting the selection criteria of this study regarding the reliability and validity of MMAS-8 including sensitivity and specificity. Meta-analysis for Cronbach's α, intraclass correlation coefficient (ICC), sensitivity and specificity to detect a patient with nonadherence to medication were performed. The pooled estimates for Cronbach's α and ICC were calculated using the random-effects weighted T transformation. A bivariate random-effects model was used to estimate pooled sensitivity and specificity.
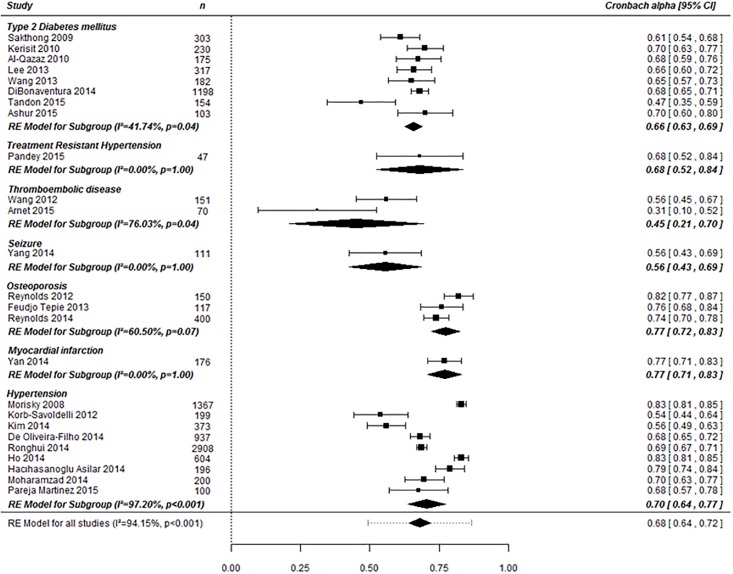
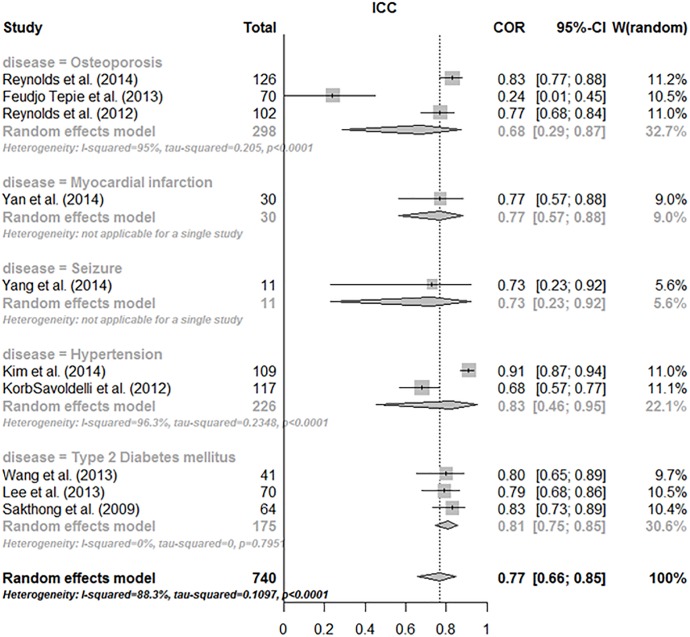
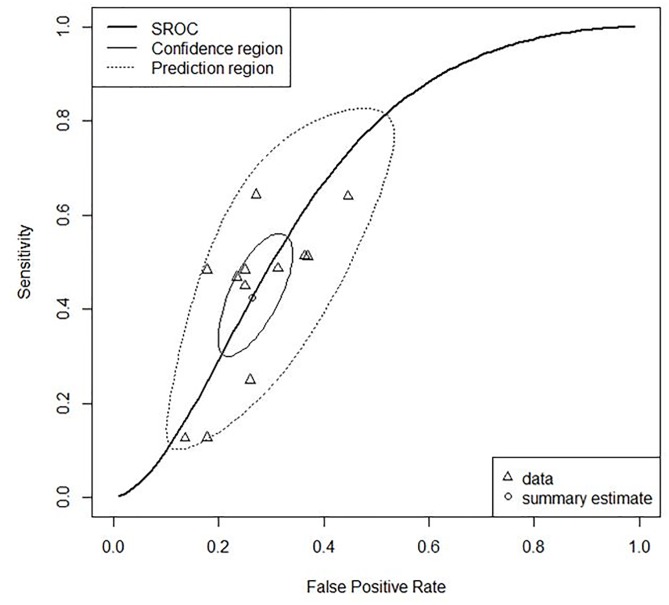
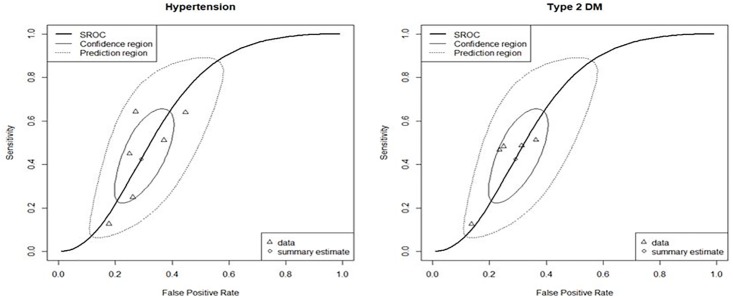
Findings: The pooled Cronbach's α estimate for type 2 diabetes group in 7 studies and osteoporosis group in 3 studies were 0.67 (95% Confidence Interval(CI), 0.65 to 0.69) and 0.77 (95% CI, 0.72 to 0.83), respectively. With regard to test-retest, the pooled ICC for type 2 diabetes group in 3 studies and osteoporosis group in 2 studies were 0.81 (95% CI, 0.75 to 0.85) and 0.80 (95% CI, 0.74 to 0.85). For a cut-off value of 6, the pooled sensitivity and specificity in 12 studies were 0.43 (95% CI, 0.33 to 0.53) and 0.73 (95% CI, 0.68 to 0.78), respectively.
Conclusions: The MMAS-8 had acceptable internal consistency and reproducibility in a few diseases like type 2 diabetes. Using the cut-off value of 6, criterion validity was not enough good to validly screen a patient with nonadherence to medication. However, this study did not calculated a pooled estimate for criterion validity using the higher values than 6 as a cut-off value since most of included individual studies did not report criterion validity based on those values.
Conflict of interest statement
Figures
References
-
- Kamran A, Sadeghieh Ahari S, Biria M, Malepour A, Heydari H. Determinants of Patient's Adherence to Hypertension Medications: Application of Health Belief Model Among Rural Patients. Ann Med Health Sci Res. 2014;4(6):922–7. Epub 2014/12/17. doi: 10.4103/2141-9248.144914 . - DOI - PMC - PubMed
-
- Parthan A, Vincze G, Morisky DE, Khan ZM. Strategies to improve adherence with medications in chronic, 'silent' diseases representing high cardiovascular risk. Expert Rev Pharmacoecon Outcomes Res. 2006;6(3):325–36. Epub 2006/06/01. doi: 10.1586/14737167.6.3.325 . - DOI - PubMed
-
- Brown MT, Bussell JK. Medication adherence: WHO cares? Mayo Clin Proc. 2011;86(4):304–14. Epub 2011/03/11. doi: 10.4065/mcp.2010.0575 . - DOI - PMC - PubMed
-
- Cohen RA, Kirzinger WK, Gindi RM. Strategies used by adults to reduce their prescription drug costs. NCHS Data Brief. 2013;(119):1–8. Epub 2013/06/08. . - PubMed
-
- Primary care physicians feel responsible for assessing patients' medication adherence, but rarely ask older patients about it directly: Primary Care. Rockville, MD: Agency for Healthcare Research and Quality; 2013. p. 20.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
