

Lamin A/C cardiomyopathy: young onset, high penetrance, and frequent need for heart transplantation
- PMID: 29095976
- PMCID: PMC5939624
- DOI: 10.1093/eurheartj/ehx596
Lamin A/C cardiomyopathy: young onset, high penetrance, and frequent need for heart transplantation
Abstract
Aims: Lamin A/C (LMNA) mutations cause familial dilated cardiomyopathy (DCM) with frequent conduction blocks and arrhythmias. We explored the prevalence, cardiac penetrance, and expressivity of LMNA mutations among familial DCM in Norway. Furthermore, we explored the risk factors and the outcomes in LMNA patients.
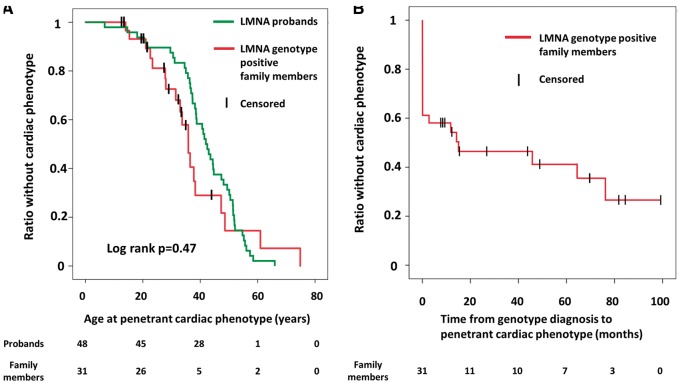
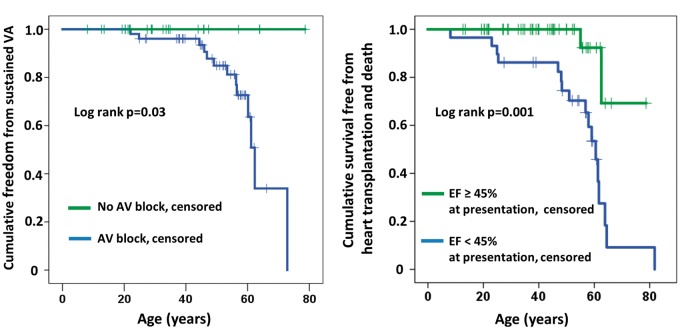
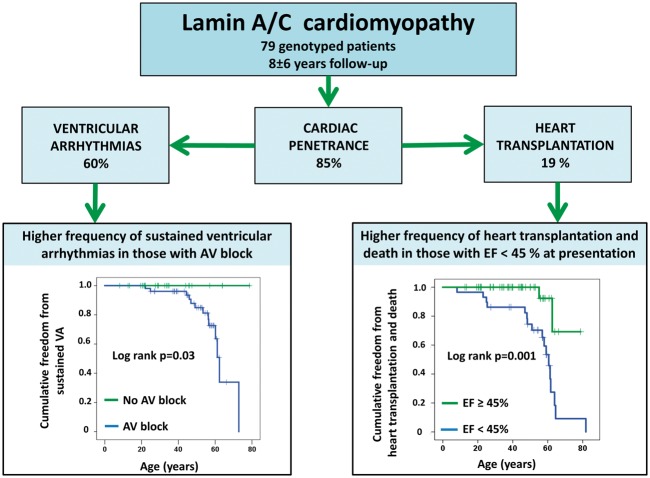
Methods and results: During 2003-15, genetic testing was performed in patients referred for familial DCM. LMNA genotype-positive subjects were examined by electrocardiography, Holter monitoring, cardiac magnetic resonance imaging, and echocardiography. A positive cardiac phenotype was defined as the presence of atrioventricular (AV) block, atrial fibrillation/flutter (AF), ventricular tachycardia (VT), and/or echocardiographic DCM. Heart transplantation was recorded and compared with non-ischaemic DCM of other origin. Of 561 unrelated familial DCM probands, 35 (6.2%) had an LMNA mutation. Family screening diagnosed an additional 93 LMNA genotype-positive family members. We clinically followed up 79 LMNA genotype-positive [age 42 ± 16 years, ejection fraction (EF) 45 ± 13%], including 44 (56%) with VT. Asymptomatic LMNA genotype-positive family members (age 31 ± 15 years) had a 9% annual incidence of a newly documented cardiac phenotype and 61% (19/31) of cardiac penetrance during 4.4 ± 2.9 years of follow-up. Ten (32%) had AV block, 7 (23%) AF, and 12 (39%) non-sustained VT. Heart transplantation was performed in 15 of 79 (19%) LMNA patients during 7.8 ± 6.3 years of follow-up.
Conclusion: LMNA mutation prevalence was 6.2% of familial DCM in Norway. Cardiac penetrance was high in young asymptomatic LMNA genotype-positive family members with frequent AV block and VT, highlighting the importance of early family screening and cardiological follow-up. Nearly 20% of the LMNA patients required heart transplantation.
Figures
Comment in
-
Lamin A/C mutations in patients with dilated cardiomyopathy.Eur Heart J. 2018 Mar 7;39(10):861-863. doi: 10.1093/eurheartj/ehx650. Eur Heart J. 2018. PMID: 29165585 No abstract available.
References
-
- van Rijsingen IA, Nannenberg EA, Arbustini E, Elliott PM, Mogensen J, Hermans-van Ast JF, van der Kooi AJ, van Tintelen JP, van den Berg MP, Grasso M, Serio A, Jenkins S, Rowland C, Richard P, Wilde AA, Perrot A, Pankuweit S, Zwinderman AH, Charron P, Christiaans I, Pinto YM.. Gender-specific differences in major cardiac events and mortality in lamin A/C mutation carriers. Eur J Heart Fail 2013;15:376–384. - PubMed
-
- Hasselberg NE, Edvardsen T, Petri H, Berge KE, Leren TP, Bundgaard H, Haugaa KH.. Risk prediction of ventricular arrhythmias and myocardial function in lamin A/C mutation positive subjects. Europace 2014;16:563–571. - PubMed
-
- Haugaa KH, Hasselberg NE, Edvardsen T.. Mechanical dispersion by strain echocardiography: a predictor of ventricular arrhythmias in subjects with lamin A/C mutations. JACC Cardiovasc Imaging 2015;8:104–106. - PubMed
-
- Priori SG, Blomström-Lundqvist C, Mazzanti A, Blom N, Borggrefe M, Camm J, Elliott PM, Fitzsimons D, Hatala R, Hindricks G, Kirchhof P, Kjeldsen K, Kuck K-H, Hernandez-Madrid A, Nikolaou N, Norekvål TM, Spaulding C, Van Veldhuisen DJ.. 2015 ESC guidelines for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death: the task force for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death of the European Society of Cardiology (ESC). Endorsed by: Association for European Paediatric and Congenital Cardiology (AEPC). Eur Heart J 2015;36:2793–2867. - PubMed
-
- van Berlo JH, de Voogt WG, van der Kooi AJ, van Tintelen JP, Bonne G, Yaou RB, Duboc D, Rossenbacker T, Heidbüchel H, de Visser M, Crijns HJGM, Pinto YM.. Meta-analysis of clinical characteristics of 299 carriers of LMNA gene mutations: do lamin A/C mutations portend a high risk of sudden death? J Mol Med (Berl) 2005;83:79–83. - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
