

Prediction of uncomplicated pregnancies in obese women: a prospective multicentre study
- PMID: 29096631
- PMCID: PMC5669007
- DOI: 10.1186/s12916-017-0956-8
Prediction of uncomplicated pregnancies in obese women: a prospective multicentre study
Abstract
Background: All obese pregnant women are considered at equal high risk with respect to complications in pregnancy and birth, and are commonly managed through resource-intensive care pathways. However, the identification of maternal characteristics associated with normal pregnancy outcomes could assist in the management of these pregnancies. The present study aims to identify the factors associated with uncomplicated pregnancy and birth in obese women, and to assess their predictive performance.
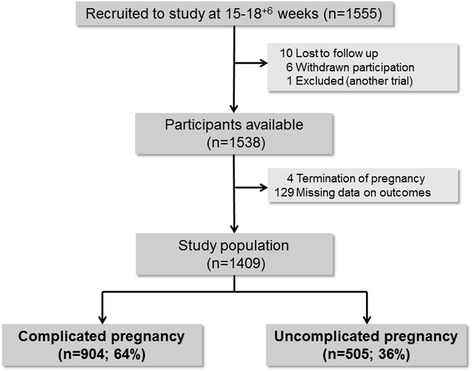
Methods: Data form obese women (BMI ≥ 30 kg/m2) with singleton pregnancies included in the UPBEAT trial were used in this analysis. Multivariable logistic regression was used to identify sociodemographic, clinical and biochemical factors at 15+0 to 18+6 weeks' gestation associated with uncomplicated pregnancy and birth, defined as delivery of a term live-born infant without antenatal or labour complications. Predictive performance was assessed using area under the receiver operating characteristic curve (AUROC). Internal validation and calibration were also performed. Women were divided into fifths of risk and pregnancy outcomes were compared between groups. Sensitivity, specificity, and positive and negative predictive values were calculated using the upper fifth as the positive screening group.
Results: Amongst 1409 participants (BMI 36.4, SD 4.8 kg/m2), the prevalence of uncomplicated pregnancy and birth was 36% (505/1409). Multiparity and increased plasma adiponectin, maternal age, systolic blood pressure and HbA1c were independently associated with uncomplicated pregnancy and birth. These factors achieved an AUROC of 0.72 (0.68-0.76) and the model was well calibrated. Prevalence of gestational diabetes, preeclampsia and other hypertensive disorders, preterm birth, and postpartum haemorrhage decreased whereas spontaneous vaginal delivery increased across the fifths of increasing predicted risk of uncomplicated pregnancy and birth. Sensitivity, specificity, and positive and negative predictive values were 38%, 89%, 63% and 74%, respectively. A simpler model including clinical factors only (no biomarkers) achieved an AUROC of 0.68 (0.65-0.71), with sensitivity, specificity, and positive and negative predictive values of 31%, 86%, 56% and 69%, respectively.
Conclusion: Clinical factors and biomarkers can be used to help stratify pregnancy and delivery risk amongst obese pregnant women. Further studies are needed to explore alternative pathways of care for obese women demonstrating different risk profiles for uncomplicated pregnancy and birth.
Keywords: Birth; Obesity; Prediction; Pregnancy outcome; Risk stratification; Uncomplicated pregnancy.
Conflict of interest statement
Authors’ information
Not applicable.
Ethics approval and consent to participate
Ethical approval was obtained from the Brighton Research Ethics Committee and all women provided informed written informed consent prior to entering the study (UK integrated research application system, reference 09/H0802/5).
Consent for publication
Not applicable.
Competing interests
All authors have completed the ICMJE uniform disclosure form at
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures

References
-
- Devlieger R, Benhalima K, Damm P, Van Assche A, Mathieu C, Mahmood T, et al. Maternal obesity in Europe: where do we stand and how to move forward?: A scientific paper commissioned by the European Board and College of Obstetrics and Gynaecology (EBCOG) Eur J Obstet Gynecol Reprod Biol. 2016;201:203–8. doi: 10.1016/j.ejogrb.2016.04.005. - DOI - PubMed
-
- NHS England . Five Year Forward View. 2016.
-
- National Maternity Review. Better Births - Improving Outcomes of Maternity Services in England. 2016. https://www.england.nhs.uk/wp-content/uploads/2016/02/national-maternity.... Accessed on 24 Nov 2016.
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
