

Observational study of lenalidomide in patients with mantle cell lymphoma who relapsed/progressed after or were refractory/intolerant to ibrutinib (MCL-004)
- PMID: 29096668
- PMCID: PMC5668956
- DOI: 10.1186/s13045-017-0537-5
Observational study of lenalidomide in patients with mantle cell lymphoma who relapsed/progressed after or were refractory/intolerant to ibrutinib (MCL-004)
Abstract
Background: The observational MCL-004 study evaluated outcomes in patients with relapsed/refractory mantle cell lymphoma who received lenalidomide-based therapy after ibrutinib failure or intolerance.
Methods: The primary endpoint was investigator-assessed overall response rate based on the 2007 International Working Group criteria.
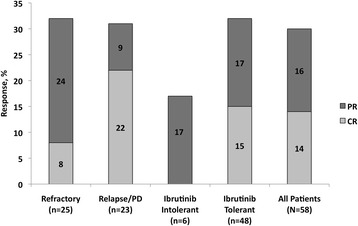
Results: Of 58 enrolled patients (median age, 71 years; range, 50-89), 13 received lenalidomide monotherapy, 11 lenalidomide plus rituximab, and 34 lenalidomide plus other treatment. Most patients (88%) had received ≥ 3 prior therapies (median 4; range, 1-13). Median time from last dose of ibrutinib to the start of lenalidomide was 1.3 weeks (range, 0.1-21.7); 45% of patients had partial responses or better to prior ibrutinib. Primary reasons for ibrutinib discontinuation were lack of efficacy (88%) and ibrutinib toxicity (9%). After a median of two cycles (range, 0-11) of lenalidomide-based treatment, 17 patients responded (8 complete responses, 9 partial responses), for a 29% overall response rate (95% confidence interval, 18-43%) and a median duration of response of 20 weeks (95% confidence interval, 2.9 to not available). Overall response rate to lenalidomide-based therapy was similar for patients with relapsed/progressive disease after previous response to ibrutinib (i.e., ≥PR) versus ibrutinib-refractory (i.e., ≤SD) patients (30 versus 32%, respectively). The most common all-grade treatment-emergent adverse events after lenalidomide-containing therapy (n = 58) were fatigue (38%) and cough, dizziness, dyspnea, nausea, and peripheral edema (19% each). At data cutoff, 28 patients have died, primarily due to mantle cell lymphoma.
Conclusion: Lenalidomide-based treatment showed clinical activity, with no unexpected toxicities, in patients with relapsed/refractory mantle cell lymphoma who previously failed ibrutinib therapy.
Trial registration: Clinicaltrials.gov identifier NCT02341781 . Date of registration: January 14, 2015.
Keywords: Ibrutinib failure; Lenalidomide; Mantle cell lymphoma.
Conflict of interest statement
Competing interests
MW reports research grants, honoraria, and nonfinancial support from Janssen, Acerta Pharma, Pharmacyclics, and Celgene; research grants and nonfinancial support from Kite Pharma; research grants from Juno Therapeutics, Amgen, Karyopharm Therapeutics, Asana BioSciences, BeiGene, Novartis, Oncoceutics, Oncternal Therapeutics, and Karus; and honoraria from BioInvent International and Adienne Pharma & Biotech.
SJS reports research funding from Celgene during the conduct of the study.
IL and TP declare that they have no competing interests.
AG reports research funding for the institution from, and was a consultant for, Celgene, Genentech, and Pharmacyclics/J&J and received honoraria from Celgene, Pharmacyclics/J&J, Acerta, and Takeda.
SR reports personal fees from Roche, Janssen, AstraZeneca, Celgene, Napp, AbbVie, and MSD.
MH was on the speaker’s bureau for Celgene and Sanofi, received honorarium from Celgene, received research funding from Takeda and Sanofi, and was a consultant for Janssen R&D.
NG reports speaker’s bureau and consultancy for Celgene, Gilead, and AbbVie; speaker’s bureau, consultancy, and research funding for PCYC and Janssen; consultancy and research funding for SGN; research funding for Genentech; and consultancy and research funding for TG Therapeutics.
CBR reports research funding from Celgene, Millennium, and Novartis.
MLCB and EB are employees of Celgene Corporation.
PM reports personal consulting fees from Celgene and Janssen/Pharmacyclics.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Dreyling M, Geisler C, Hermine O, Kluin-Nelemans HC, Le Gouill S, Rule S, et al: Newly diagnosed and relapsed mantle cell lymphoma: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol 2014;25 Suppl 3:iii83-iii92. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
