

Sex Chromosome Complement Defines Diffuse Versus Focal Angiotensin II-Induced Aortic Pathology
- PMID: 29097367
- PMCID: PMC5864127
- DOI: 10.1161/ATVBAHA.117.310035
Sex Chromosome Complement Defines Diffuse Versus Focal Angiotensin II-Induced Aortic Pathology
Abstract
Objective: Aortic pathologies exhibit sexual dimorphism, with aneurysms in both the thoracic and abdominal aorta (ie, abdominal aortic aneurysm [AAA]) exhibiting higher male prevalence. Women have lower prevalence of aneurysms, but when they occur, aneurysms progress rapidly. To define mechanisms for these sex differences, we determined the role of sex chromosome complement and testosterone on the location and progression of angiotensin II (AngII)-induced aortic pathologies.
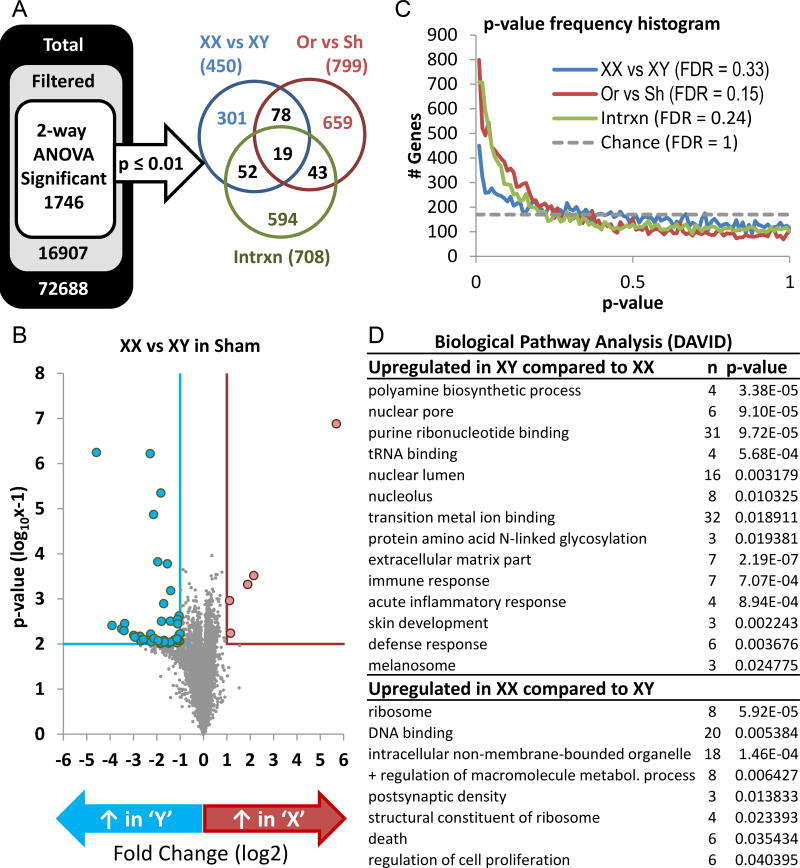
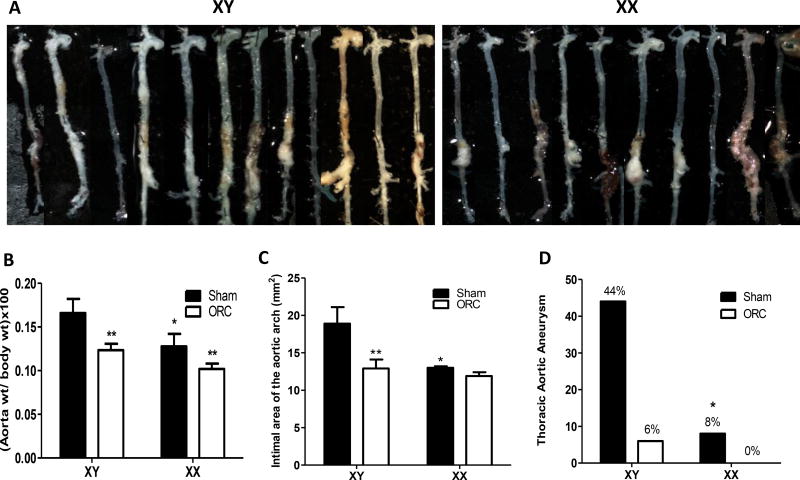
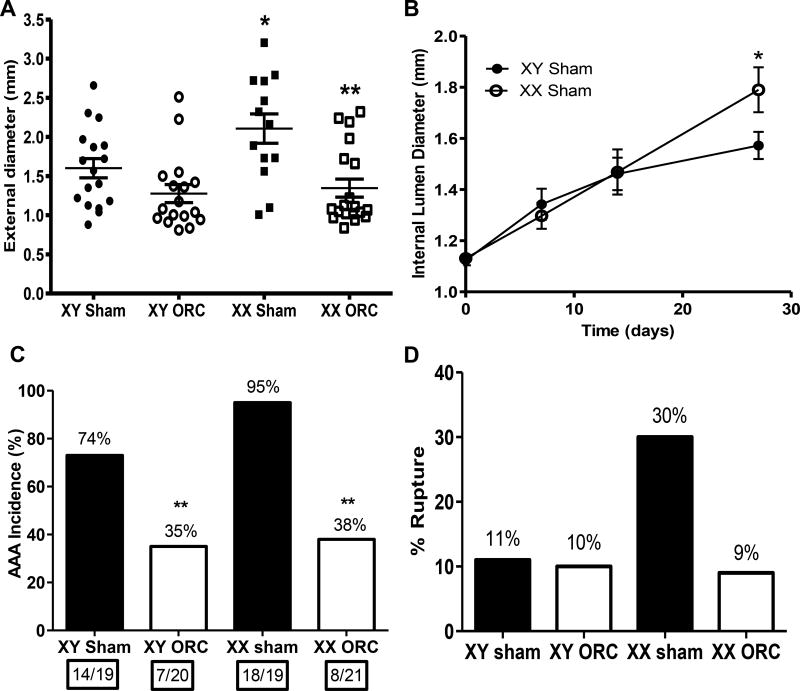
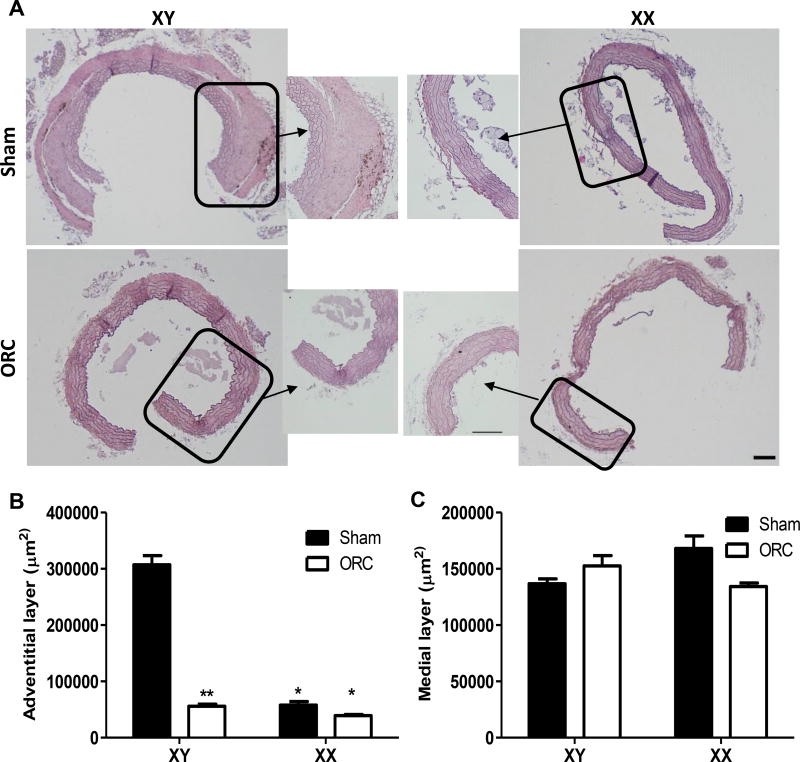
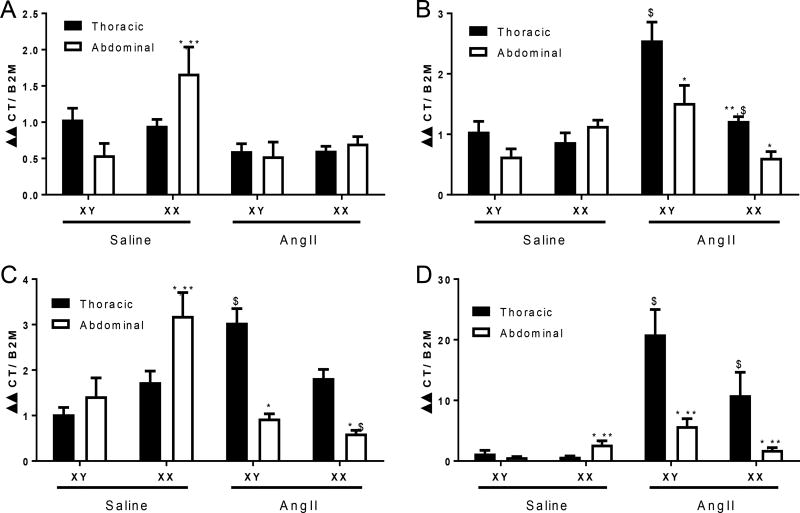
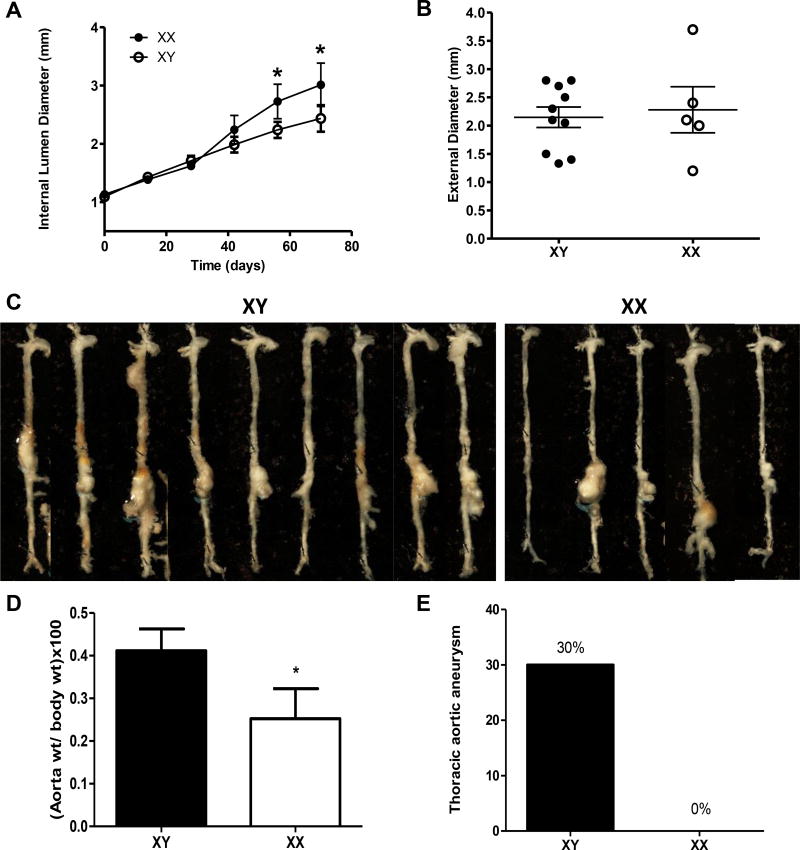
Approach and results: We used transgenic male mice expressing Sry (sex-determining region Y) on an autosome to create Ldlr (low-density lipoprotein receptor)-deficient male mice with an XY or XX sex chromosome complement. Transcriptional profiling was performed on abdominal aortas from XY or XX males, demonstrating 1746 genes influenced by sex chromosomes or sex hormones. Males (XY or XX) were either sham-operated or orchiectomized before AngII infusions. Diffuse aortic aneurysm pathology developed in XY AngII-infused males, whereas XX males developed focal AAAs. Castration reduced all AngII-induced aortic pathologies in XY and XX males. Thoracic aortas from AngII-infused XY males exhibited adventitial thickening that was not present in XX males. We infused male XY and XX mice with either saline or AngII and quantified mRNA abundance of key genes in both thoracic and abdominal aortas. Regional differences in mRNA abundance existed before AngII infusions, which were differentially influenced by AngII between genotypes. Prolonged AngII infusions resulted in aortic wall thickening of AAAs from XY males, whereas XX males had dilated focal AAAs.
Conclusions: An XY sex chromosome complement mediates diffuse aortic pathology, whereas an XX sex chromosome complement contributes to focal AngII-induced AAAs.
Keywords: aneurysm; aorta; pathology; sex chromosomes; testosterone.
© 2017 American Heart Association, Inc.
Figures
Comment in
-
X Marks the Spot: The Profound Impact of Sex on Aortic Disease.Arterioscler Thromb Vasc Biol. 2018 Jan;38(1):9-11. doi: 10.1161/ATVBAHA.117.310433. Arterioscler Thromb Vasc Biol. 2018. PMID: 29282246 Free PMC article. No abstract available.
References
-
- Roman MJ, Devereux RB, Preiss LR, et al. Gen TACI. Associations of age and sex with marfan phenotype: The national heart, lung, and blood institute gentac (genetically triggered thoracic aortic aneurysms and cardiovascular conditions) registry. Circulation. Cardiovascular genetics. 2017;10 - PMC - PubMed
-
- Pleumeekers HJ, Hoes AW, van der Does E, van Urk H, Hofman A, de Jong PT, Grobbee DE. Aneurysms of the abdominal aorta in older adults. The rotterdam study. American journal of epidemiology. 1995;142:1291–1299. - PubMed
-
- Zarrouk M, Holst J, Malina M, Lindblad B, Wann-Hansson C, Rosvall M, Gottsater A. The importance of socioeconomic factors for compliance and outcome at screening for abdominal aortic aneurysm in 65-year-old men. Journal of vascular surgery. 2013;58:50–55. - PubMed
-
- Svensjo S, Bjorck M, Wanhainen A. Current prevalence of abdominal aortic aneurysm in 70-year-old women. The British journal of surgery. 2013;100:367–372. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
