

Clinical Applications of Contrast-Enhanced Perfusion MRI Techniques in Gliomas: Recent Advances and Current Challenges
- PMID: 29097933
- PMCID: PMC5612612
- DOI: 10.1155/2017/7064120
Clinical Applications of Contrast-Enhanced Perfusion MRI Techniques in Gliomas: Recent Advances and Current Challenges
Abstract
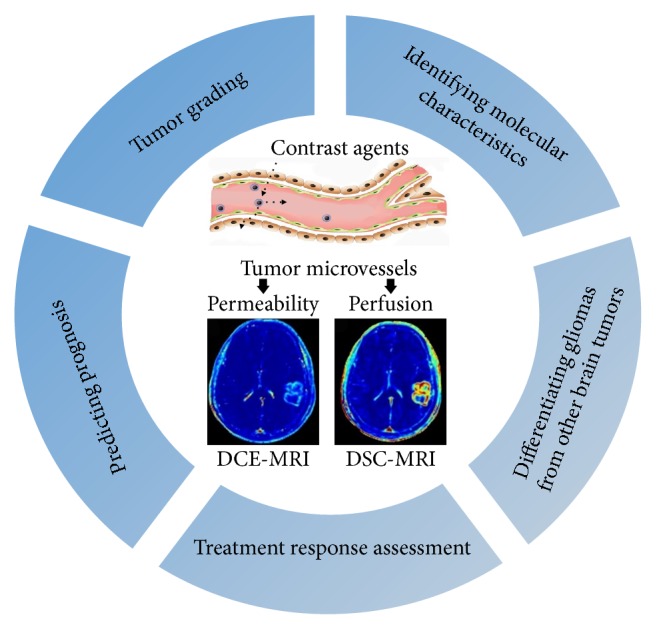
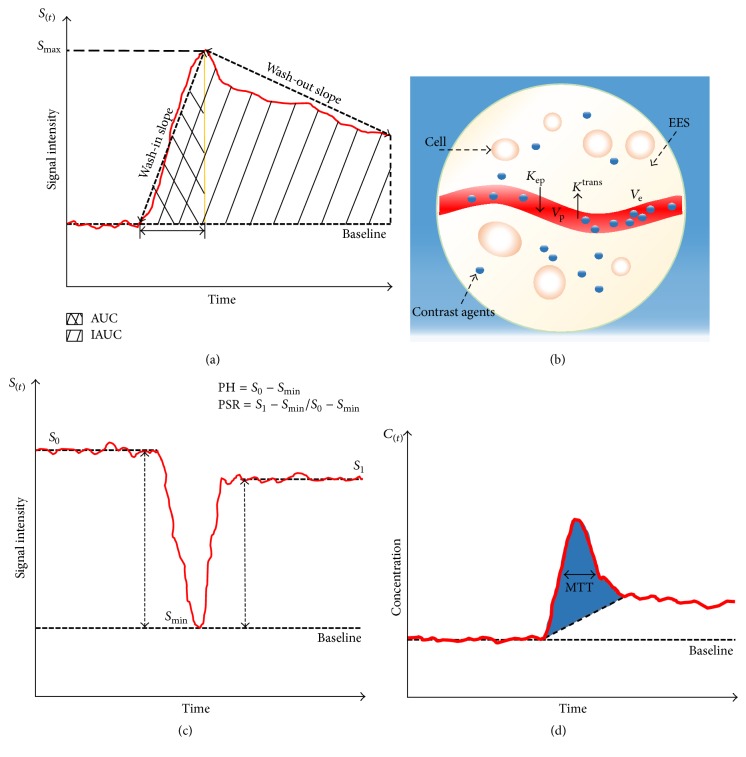
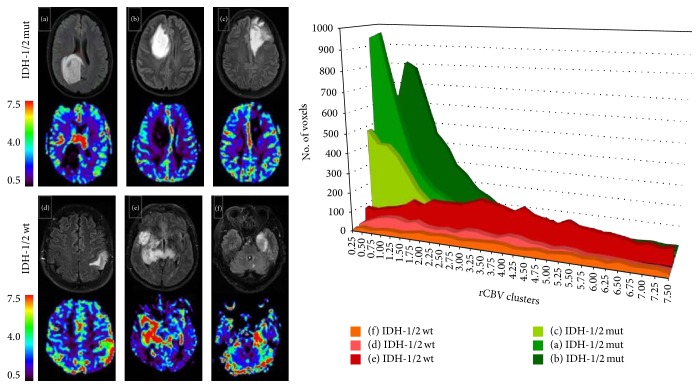
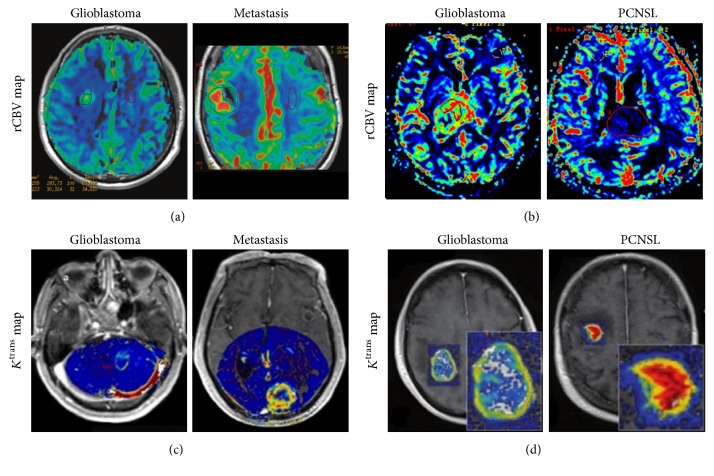
Gliomas possess complex and heterogeneous vasculatures with abnormal hemodynamics. Despite considerable advances in diagnostic and therapeutic techniques for improving tumor management and patient care in recent years, the prognosis of malignant gliomas remains dismal. Perfusion-weighted magnetic resonance imaging techniques that could noninvasively provide superior information on vascular functionality have attracted much attention for evaluating brain tumors. However, nonconsensus imaging protocols and postprocessing analysis among different institutions impede their integration into standard-of-care imaging in clinic. And there have been very few studies providing a comprehensive evidence-based and systematic summary. This review first outlines the status of glioma theranostics and tumor-associated vascular pathology and then presents an overview of the principles of dynamic contrast-enhanced MRI (DCE-MRI) and dynamic susceptibility contrast-MRI (DSC-MRI), with emphasis on their recent clinical applications in gliomas including tumor grading, identification of molecular characteristics, differentiation of glioma from other brain tumors, treatment response assessment, and predicting prognosis. Current challenges and future perspectives are also highlighted.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
