

New agents in the Treatment of Myeloma Bone Disease
- PMID: 29098361
- PMCID: PMC5805798
- DOI: 10.1007/s00223-017-0351-7
New agents in the Treatment of Myeloma Bone Disease
Abstract
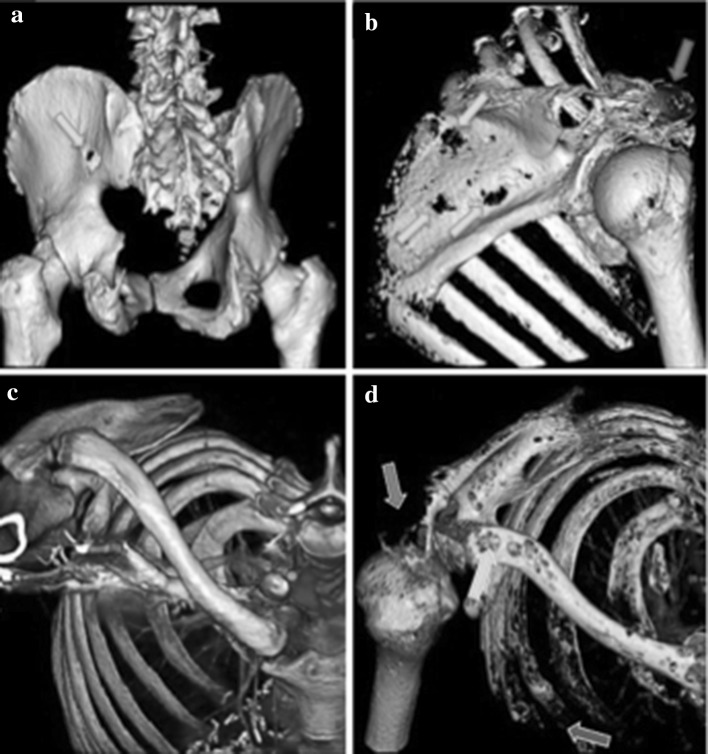
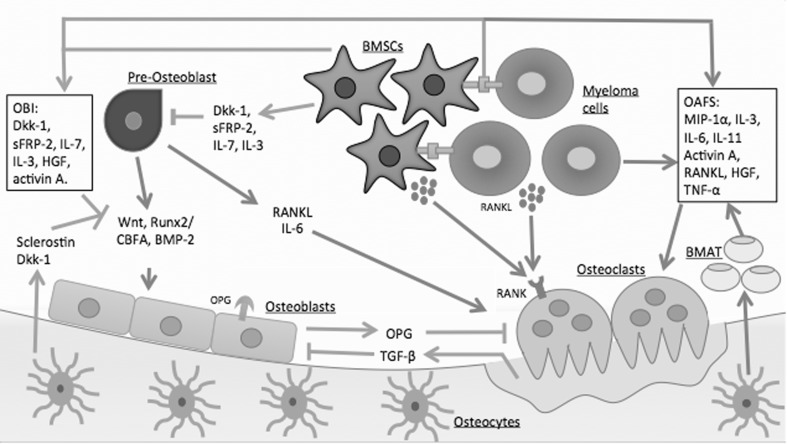
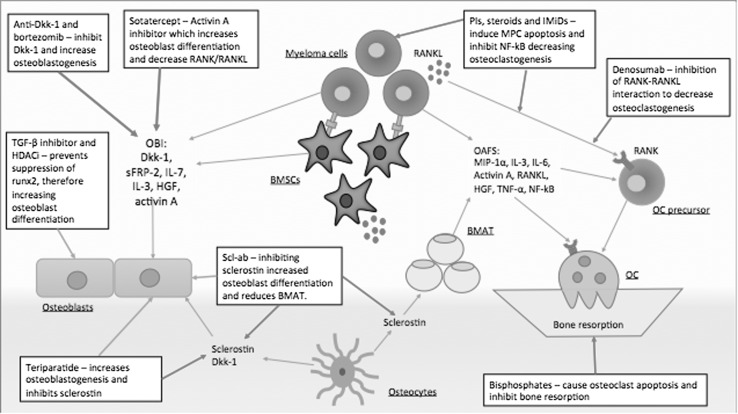
Patients with multiple myeloma develop a devastating bone disease driven by the uncoupling of bone remodelling, excess osteoclastic bone resorption and diminished osteoblastic bone formation. The bone phenotype is typified by focal osteolytic lesions leading to pathological fractures, hypercalcaemia and other catastrophic bone events such as spinal cord compression. This causes bone pain, impaired functional status, decreased quality of life and increased mortality. Early in the disease, malignant plasma cells occupy a niche environment that encompasses their interaction with other key cellular components of the bone marrow microenvironment. Through these interactions, osteoclast-activating factors and osteoblast inhibitory factors are produced, which together uncouple the dynamic process of bone remodelling, leading to net bone loss and focal osteolytic lesions. Current management includes antiresorptive therapies, i.e. bisphosphonates, palliative support and orthopaedic interventions. Bisphosphonates are the mainstay of treatment for myeloma bone disease (MBD), but are only partially effective and do have some significant disadvantages; for example, they do not lead to the repair of existing bone destruction. Thus, newer agents to prevent bone destruction and also promote bone formation and repair existing lesions are warranted. This review summarises novel ways that MBD is being therapeutically targeted.
Keywords: Anabolic agents; Antiresorptive agents; Bone remodelling; Myeloma; Myeloma bone disease.
Figures

References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
