

Review
doi: 10.1007/s00415-017-8652-3.
Epub 2017 Nov 2.
Neurological update: gliomas and other primary brain tumours in adults
Affiliations
- PMID: 29098416
- PMCID: PMC5834564
- DOI: 10.1007/s00415-017-8652-3
Item in Clipboard
Review
Neurological update: gliomas and other primary brain tumours in adults
J Neurol.
2018 Mar.
Abstract
The emerging understanding of molecular changes in a wide range of brain tumours has led to a significant shift in how these tumours are diagnosed, managed and treated. This article will provide a hands-on overview of the relevant biomarkers and their association with newly defined biological tumour entities.
Keywords: ATRX; Astrocytoma; BRAF; BRAF inhibitor; EGFR; Ependymoma; Glioblastoma; Histone; IDH; MGMT; Mutation; Oligodendroglioma; TERT; Temozolomide; Tumour heterogeneity.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
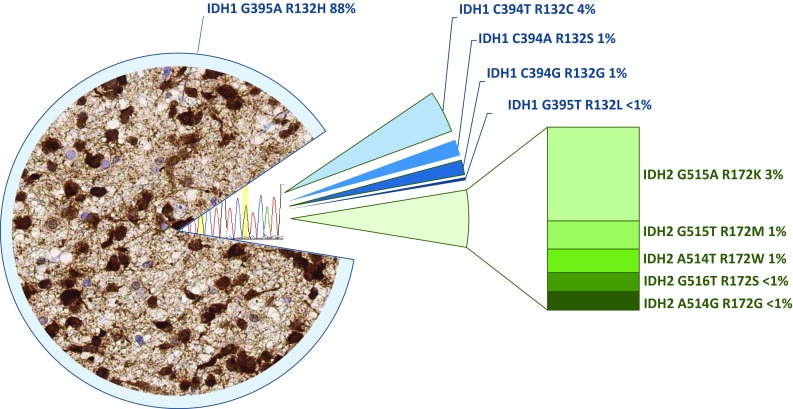
Frequency of IDH1 and IDH2 mutations in a cohort of 747 oligodendroglial and astrocytic tumours (extracted from the data in [19]) and two added rare IDH2 mutations. The left part of the graph shows a typical histological image of immunostaining in an IDH1 R132H mutant astrocytoma with an antibody detecting this specific mutation. Approximately 90% of all IDH-mutant tumours and 95% of IDH1 mutations are detected with this antibody. The remaining IDH1 mutations and all IDH2 mutations are most commonly detected by sequencing the hotspot on codon 132 (IDH1) and 172 (IDH2) (right part of the figure). The frequency of IDH-mutant gliomas rapidly decreases with the age of the patient. The probability of an alternative IDH mutation is < 6% in a 50-year-old patient and decreases to < 1% in patients aged > 54 years [7]
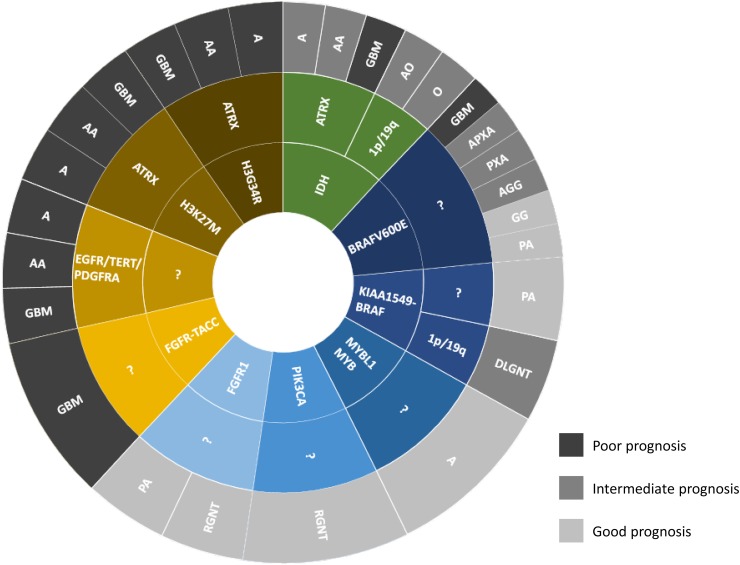
Simplified scheme of known genetic alterations in the most common glial and glioneuronal tumours. The inner circle shows the presumed driver mutation, such as IDH (green), histone H3.3 K27M, G34R, FGFR–TACC fusion (brown), or BRAF alterations (dark blue), MYB/MYBL1, PIK3CA and FGFR1 (lighter blue shades). The middle circle shows known additional mutations that are associated with the respective tumour entities. For example, in the group of IDH-mutant tumours, the 1p/19q codeletion defines the oligodendroglioma, whilst the ATRX mutation defines the IDH-mutant astrocytoma. The IDH-wildtype glioblastoma (light brown) currently does not have a defined driver mutation, but it contains a combination of signature alterations such as EGFR or PDRGRA amplifications, TERT promoter mutation and others. The outer circle shows the histological diagnosis with the abbreviations corresponding to the following histological entities: A astrocytoma, AA anaplastic astrocytoma, GBM glioblastoma, O oligodendroglioma, AO anaplastic oligodendroglioma, PXA pleomorphic xanthoastrocytoma, APXA anaplastic pleomorphic xanthoastrocytoma, GG ganglioglioma, AGG anaplastic ganglioglioma, PA pilocytic astrocytoma, DLGNT diffuse leptomeningeal glioneuronal tumour, RGNT rosette forming glioneuronal tumour. The grey shades for each histological diagnosis indicate the prognosis: light grey corresponds to good prognosis and darkest grey corresponds to poorest prognosis. Note that tumours with identical histological diagnoses, depending on their underlying genetic alteration, can show different biological behaviour and thus have a different prognosis. For example, H3 K27M mutant gliomas (brown) can have a low- or high-grade histological appearance but all have a poor prognosis. Conversely, BRAF-mutant gliomas cover a wide spectrum prognoses ranging from benign to highly malignant tumours. The diagram is for illustrative purposes and does not reflect frequencies of any of these entities
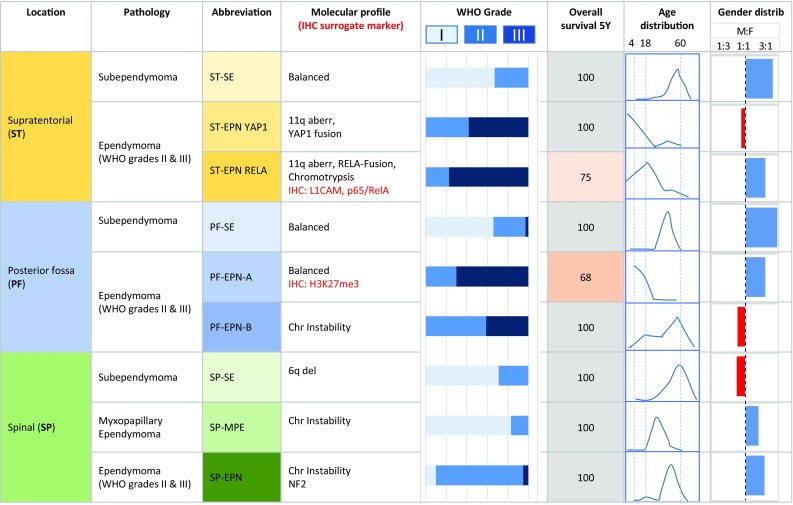
Diagrammatic summary of the most recent molecular subgrouping of ependymomas based on DNA methylation patterns [30, 31]. These molecular subgroups are genetically, epigenetically, transcriptionally, demographically and clinically distinct. Three topographically distinct overarching groups are identified, supratentorial (ST), posterior fossa (PF) and spinal (SP). Within each group there are three molecularly distinct molecular subgroups. Two of these nine groups are characterised by poor 5 year survival. The molecular profile column includes the immunohistochemically detectable surrogate markers of the PF-EPN-A and ST-EPN-RELA. All spinal tumours show favourable outcome when surgically completely removed
References
-
- Banerjee A, Jakacki RI, Onar-Thomas A, Wu S, Nicolaides T, Young Poussaint T, Fangusaro J, Phillips J, Perry A, Turner D, Prados M, Packer RJ, Qaddoumi I, Gururangan S, Pollack IF, Goldman S, Doyle LA, Stewart CF, Boyett JM, Kun LE, Fouladi M. A phase I trial of the MEK inhibitor selumetinib (AZD6244) in pediatric patients with recurrent or refractory low-grade glioma: a Pediatric Brain Tumor Consortium (PBTC) study. Neuro Oncol. 2017;19:9. doi: 10.1093/neuonc/now282. - DOI - PMC - PubMed
-
- Capper D, Weissert S, Balss J, Habel A, Meyer J, Jager D, Ackermann U, Tessmer C, Korshunov A, Zentgraf H, Hartmann C, von Deimling A. Characterization of R132H mutation-specific IDH1 antibody binding in brain tumors. Brain Pathol. 2010;20:245–254. doi: 10.1111/j.1750-3639.2009.00352.x. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
