

Carotid-cavernous fistula: current concepts in aetiology, investigation, and management
- PMID: 29099499
- PMCID: PMC5811734
- DOI: 10.1038/eye.2017.240
Carotid-cavernous fistula: current concepts in aetiology, investigation, and management
Abstract
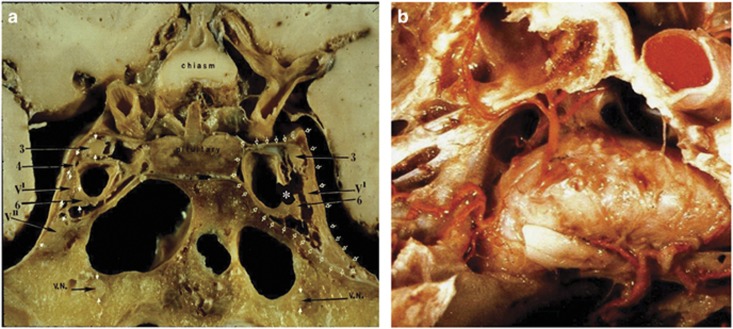
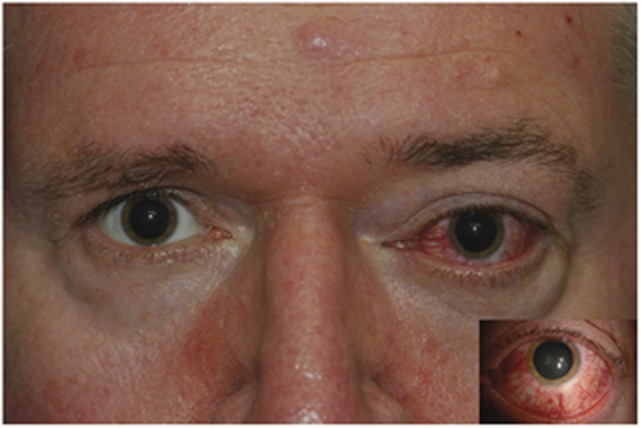
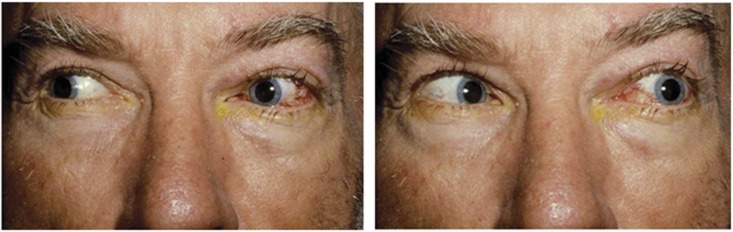
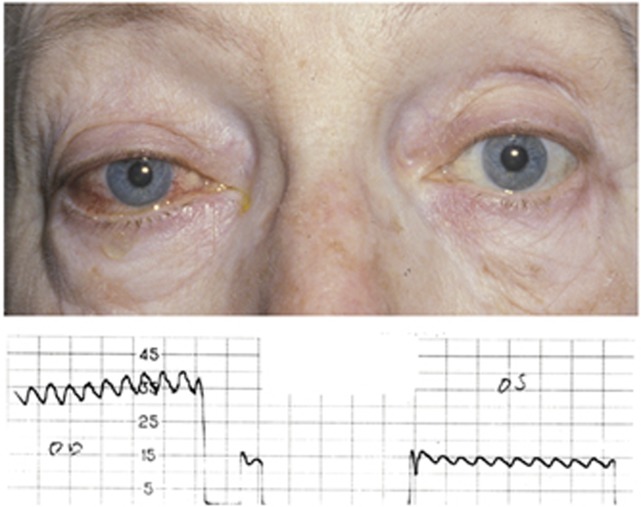
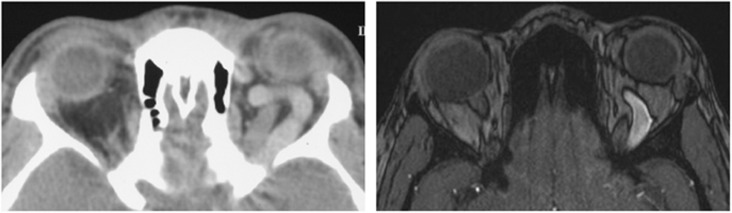
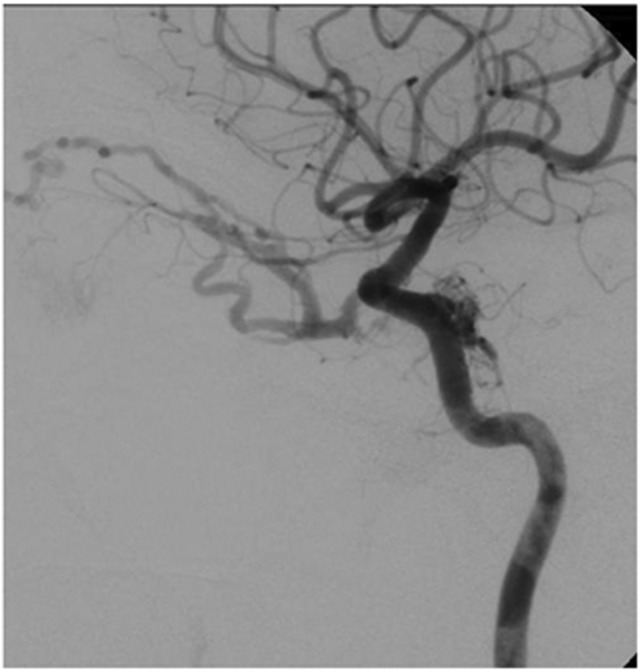
A carotid-cavernous fistula (CCF) is an abnormal communication between arteries and veins within the cavernous sinus and may be classified as either direct or dural. Direct CCFs are characterized by a direct connection between the internal carotid artery (ICA) and the cavernous sinus, whereas dural CCFs result from an indirect connection involving cavernous arterial branches and the cavernous sinus. Direct CCFs frequently are traumatic in origin and also may be caused by rupture of an ICA aneurysm within the cavernous sinus, Ehlers-Danlos syndrome type IV, or iatrogenic intervention. Causes of dural CCFs include hypertension, fibromuscular dysplasia, Ehlers-Danlos type IV, and dissection of the ICA. Evaluation of a suspected CCF often involves non-invasive imaging techniques, including standard tonometry, pneumotonometry, ultrasound, computed tomographic scanning and angiography, and/or magnetic resonance imaging and angiography, but the gold standard for classification and diagnosis remains digital subtraction angiography. When a direct CCF is confirmed, first-line treatment is endovascular intervention, which may be accomplished using detachable balloons, coils, liquid embolic agents, or a combination of these tools. As dural CCFs often resolve spontaneously, low-risk cases may be managed conservatively. When invasive treatment is warranted, endovascular intervention or stereotactic radiosurgery may be performed. Modern endovascular techniques offer the ability to successfully treat CCFs with a low morbidity and virtually no mortality.
Conflict of interest statement
The authors declare no conflict of interest.
Figures





Comment in
-
Comment on: Carotid-cavernous fistula: current concepts in aetiology, investigation and management.Eye (Lond). 2018 Oct;32(10):1675-1680. doi: 10.1038/s41433-018-0112-5. Epub 2018 May 18. Eye (Lond). 2018. PMID: 29773880 Free PMC article. No abstract available.
-
Reply to 'Comment on: Carotid-cavernous fistula: current concepts in aetiology, investigation and management'.Eye (Lond). 2018 Oct;32(10):1676. doi: 10.1038/s41433-018-0113-4. Epub 2018 May 22. Eye (Lond). 2018. PMID: 29786088 Free PMC article. No abstract available.
References
-
- Barrow DL, Spector RH, Braun IF, Landman JA, Tindall SC, Tindall GT. Classification and treatment of spontaneous carotid-cavernous fistulas. J Neurosurg 1985; 62(2): 248–256. - PubMed
-
- Kashiwagi S, Tsuchida E, Goto K, Shiroyama Y, Yamashita T, Takahasi M et al. Balloon occlusion of a spontaneous carotid-cavernous fistula in Ehlers-Danlos syndrome type IV. Surg Neurol 1993; 39(3): 187–190. - PubMed
-
- Masson-Roy J, Savard M, Mackey A. Carotid cavernous fistula in a patient with type IV Ehlers-Danlos syndrome. Can J Neurol Sci 2017; 44(4): 1–2. - PubMed
-
- Schievink WI, Piepgras DG, Earnest F, Gordon H. Spontaneous carotid-cavernous fistulae in Ehlers-Danlos syndrome type IV: case report. J Neurosurg 1991; 74(6): 991–998. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
