

Toward noninvasive monitoring of ongoing electrical activity of human uterus and fetal heart and brain
- PMID: 29100065
- PMCID: PMC5697525
- DOI: 10.1016/j.clinph.2017.08.026
Toward noninvasive monitoring of ongoing electrical activity of human uterus and fetal heart and brain
Abstract
Objective: To evaluate whether a full-coverage fetal-maternal scanner can noninvasively monitor ongoing electrophysiological activity of maternal and fetal organs.
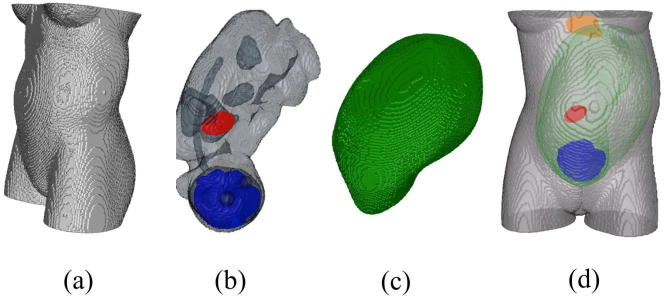
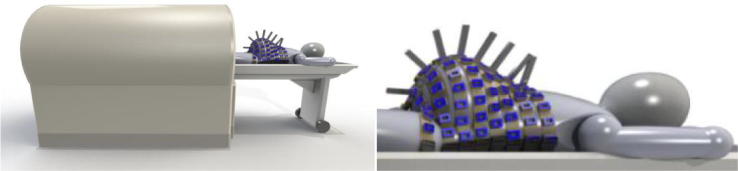
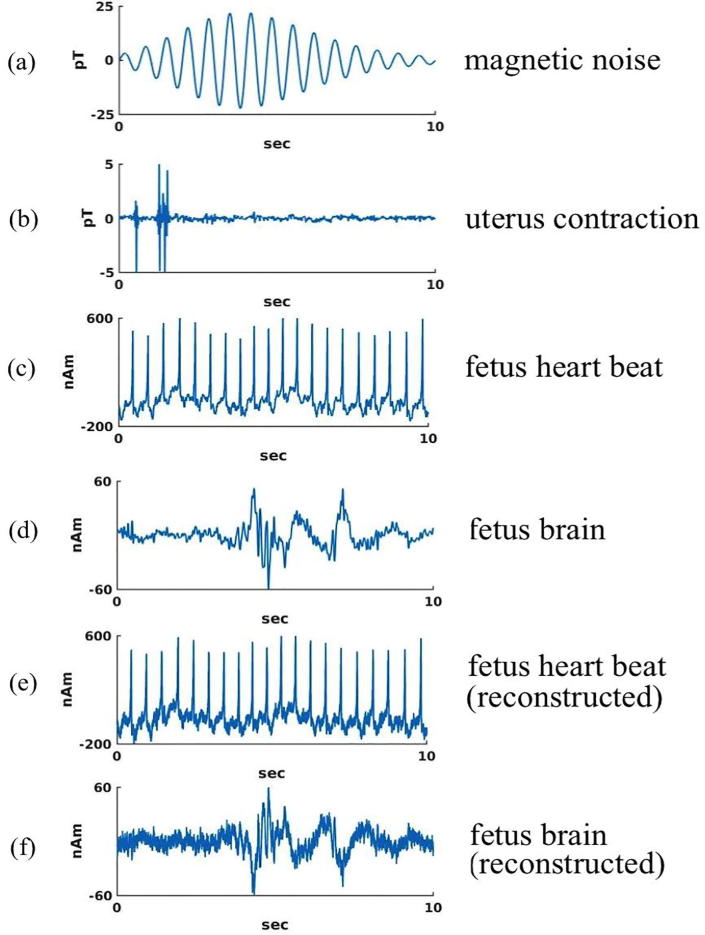
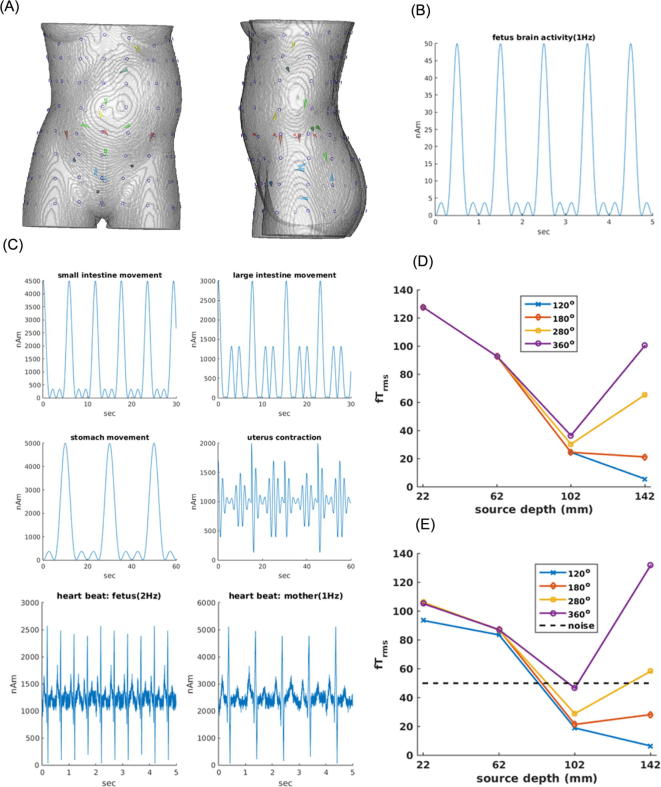
Methods: A simulation study was carried out for a scanner with an array of magnetic field sensors placed all around the torso from the chest to the hip within a horizontal magnetic shielding enclosure. The magnetic fields from internal organs and an external noise source were computed for a pregnant woman with a 35-week old fetus. Signal processing methods were used to reject the external and internal interferences, to visualize uterine activity, and to detect activity of fetal heart and brain.
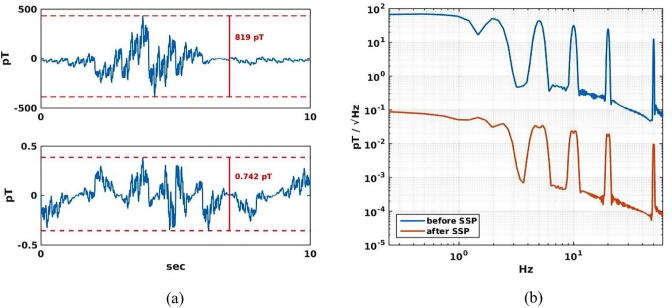
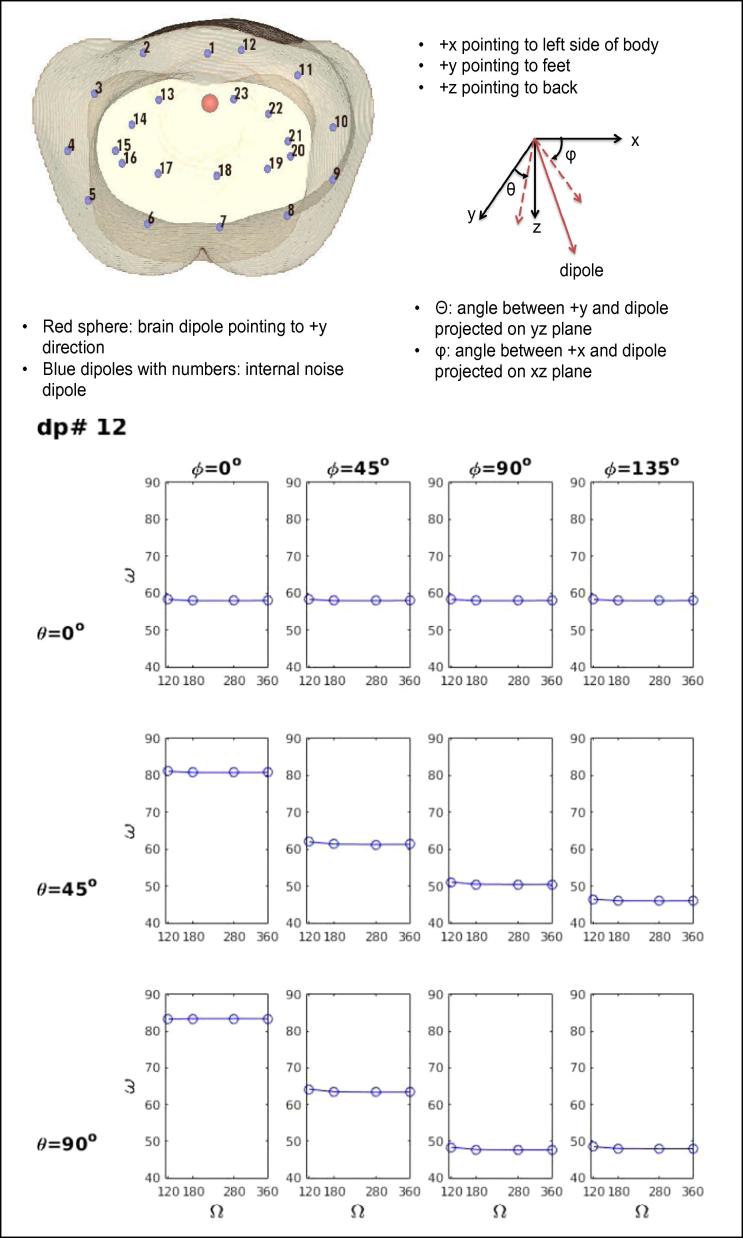
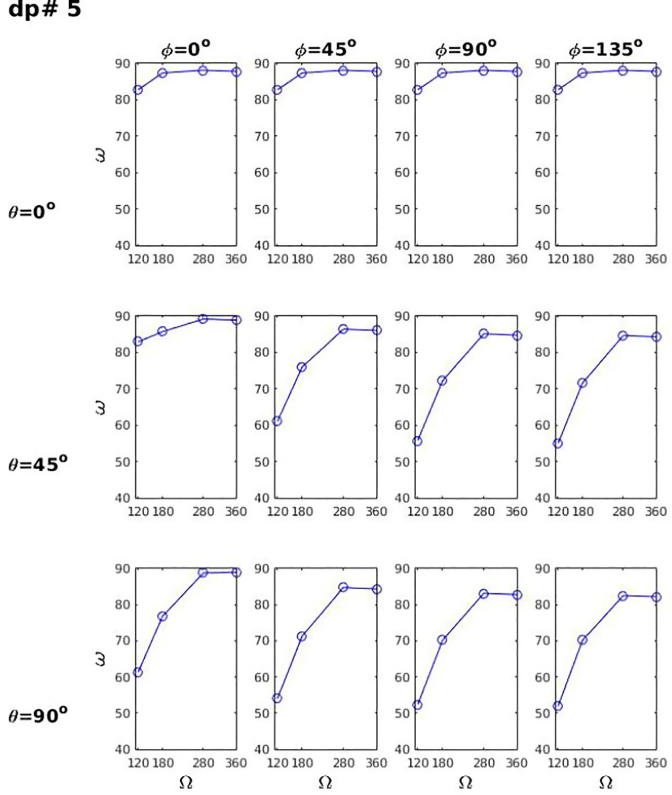
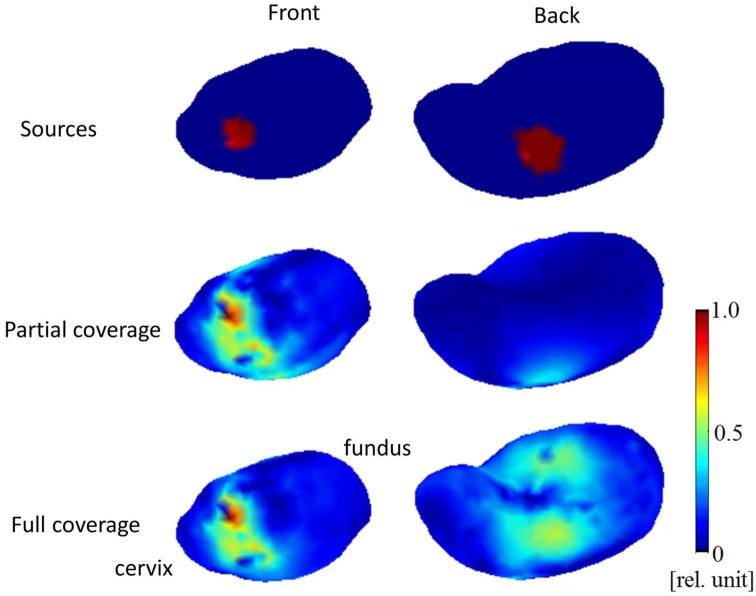
Results: External interference was reduced by a factor of 1000, sufficient for detecting signals from internal organs when combined with passive and active shielding. The scanner rejects internal interferences better than partial-coverage arrays. It can be used to estimate currents around the uterus. It clearly detects spontaneous activity from the fetal heart and brain without averaging and weaker evoked brain activity at all fetal head positions after averaging.
Conclusion: The simulated device will be able to monitor the ongoing activity of the fetal and maternal organs.
Significance: This type of scanner may become a novel tool in fetal medicine.
Keywords: Electrocardiography (ECG); Electroencephalography (EEG); Electrohysterography (EHG); Magnetocardiography (MCG); Magnetoencephalography (MEG); Prenatal medicine.
Copyright © 2017 International Federation of Clinical Neurophysiology. Published by Elsevier B.V. All rights reserved.
Figures

Comment in
-
Reply to "Prospective advances in fetal biomagnetometry - Challenges remain".Clin Neurophysiol. 2018 Feb;129(2):505-506. doi: 10.1016/j.clinph.2017.12.030. Epub 2017 Dec 28. Clin Neurophysiol. 2018. PMID: 29307450 No abstract available.
-
Prospective advances in fetal biomagnetometry - Challenges remain.Clin Neurophysiol. 2018 Feb;129(2):503-504. doi: 10.1016/j.clinph.2017.11.031. Epub 2017 Dec 28. Clin Neurophysiol. 2018. PMID: 29325857 No abstract available.
References
-
- Alem O., Sander T.H., Mhaskar R., LeBlanc J., Eswaran H., Steinhoff U., Okada Y., Kitching J., Trahms L., Knappe S. Fetal magnetocardiography measurements with an array of microfabricated optically pumped magnetometers. Phys Med Biol. 2015;60:4797–4811. - PubMed
-
- Bakker J.J.H., Verhoeven C.J.M., Janssen P.F., van Lith J.M., van Uodgaarden E.D., Boemenkamp K.W.M., Pasatsonis D.N.M., Willem B., Mol J., van der Post J.A.M. Outcomes after internal versus external tocodynamometry for monitoring labor. New Engl J Med. 2010;362:306–313. - PubMed
-
- Bibin L., Anquez J., Alcalde J.P., Boubekeur T., Angelini E., Bloch I. Whole body pregnant woman modeling by digital geometry processing with detailed utero-fetal unit based on medical images. IEEE Trans Biomed Eng. 2010;57:2346–2358. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
