

Low sensitivity of qSOFA, SIRS criteria and sepsis definition to identify infected patients at risk of complication in the prehospital setting and at the emergency department triage
- PMID: 29100549
- PMCID: PMC5670696
- DOI: 10.1186/s13049-017-0449-y
Low sensitivity of qSOFA, SIRS criteria and sepsis definition to identify infected patients at risk of complication in the prehospital setting and at the emergency department triage
Abstract
Background: Sepsis is defined as life-threatening organ dysfunction caused by a host response to infection. The quick SOFA (qSOFA) score has been recently proposed as a new bedside clinical score to identify patients with suspected infection at risk of complication (intensive care unit (ICU) admission, in-hospital mortality). The aim of this study was to measure the sensitivity of the qSOFA score, SIRS criteria and sepsis definitions to identify the most serious sepsis cases in the prehospital setting and at the emergency department (ED) triage.
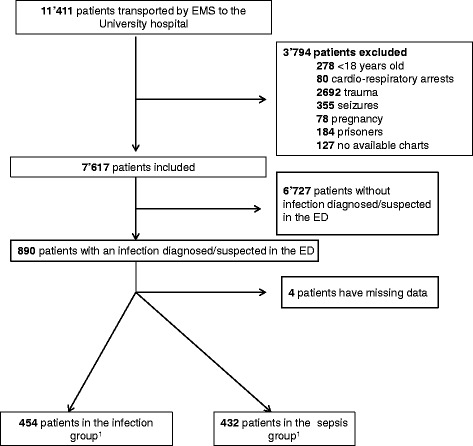
Methods: We performed a retrospective study of all patients transported by emergency medical services (EMS) to the Lausanne University Hospital (CHUV) over twelve months. All patients with a suspected or proven infection after the ED workup were included. We retrospectively analysed the sensitivity of the qSOFA score (≥2 criteria), SIRS criteria (≥2 clinical criteria) and sepsis definition (SIRS criteria + one sign of organ dysfunction or hypoperfusion) in the pre-hospital setting and at the ED triage as predictors of ICU admission, ICU stay of ≥3 days and early (i.e. 48 h) mortality. No direct comparison between the three tools was attempted.
Results: Among 11,411 patients transported to the University hospital, 886 (7.8%) were included. In the pre-hospital setting, the sensitivity of qSOFA reached 36.3% for ICU admission, 17.4% for ICU stay of three days or more and 68.0% for 48 h mortality. The sensitivity of SIRS criteria reached 68.8% for ICU admission, 74.6% for ICU stay of three days or more and 64.0% for 48 h mortality. The sensitivity of sepsis definition did not reach 60% for any outcome. At ED triage, the sensitivity of qSOFA reached 31.2% for ICU admission, 30.5% for ICU stay of ≥3 days and 60.0% for mortality at 48 h. The sensitivity of SIRS criteria reached 58.8% for ICU admission, 57.6% for ICU stay of ≥3 days 80.0% for mortality at 48 h. The sensitivity of sepsis definition reached 60.0% for 48 h mortality.
Discussion: Incidence of sepsis in the ED among patients transported by ambulance was 3.8 percent. This rate, associated to the mortality of sepsis, confirms the necessity to dispose of a test to early identify those patients.
Conclusion: The sensitivity performance of all three tools was suboptimal. The qSOFA score, SIRS criteria and sepsis definition have low identification sensitivity in selecting septic patients in the pre-hospital setting or upon arrival in the ED at risk of complication.
Keywords: Emergency department; Prehospital care; Quick SOFA score; Sepsis; Septic shock; qSOFA.
Conflict of interest statement
Ethics approval and consent to participate
The study was approved by the local Institutional Review and Ethics Boards of the University of Lausanne (Commission cantonale d’éthique de la recherche sur l’être humain (CER_VD), protocol 186/15). No authorisation from patients was required as ours was a retrospective study on de-identified lists of patients.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Bone RC, Balk RA, Cerra FB, Dellinger RP, Fein AM, Knaus WA, Schein RM, Sibbald WJ. Definitions for sepsis and organ failure and guidelines for the use of innovative therapies in sepsis. The ACCP/SCCM consensus conference committee. American College of Chest Physicians/Society of Critical Care Medicine. Chest. 1992;101(6):1644–1655. doi: 10.1378/chest.101.6.1644. - DOI - PubMed
-
- Dellinger RP, Levy MM, Rhodes A, Annane D, Gerlach H, Opal SM, Sevransky JE, Sprung CL, Douglas IS, Jaeschke R, et al. Surviving sepsis campaign: international guidelines for management of severe sepsis and septic shock: 2012. Crit Care Med. 2013;41(2):580–637. doi: 10.1097/CCM.0b013e31827e83af. - DOI - PubMed
-
- Glickman SW, Cairns CB, Otero RM, Woods CW, Tsalik EL, Langley RJ, van Velkinburgh JC, Park LP, Glickman LT, Fowler VG, Jr, et al. Disease progression in hemodynamically stable patients presenting to the emergency department with sepsis. Acad Emerg Med. 2010;17(4):383–390. doi: 10.1111/j.1553-2712.2010.00664.x. - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
