

Intersociety policy statement on the use of whole-exome sequencing in the critically ill newborn infant
- PMID: 29100554
- PMCID: PMC5670717
- DOI: 10.1186/s13052-017-0418-0
Intersociety policy statement on the use of whole-exome sequencing in the critically ill newborn infant
Abstract
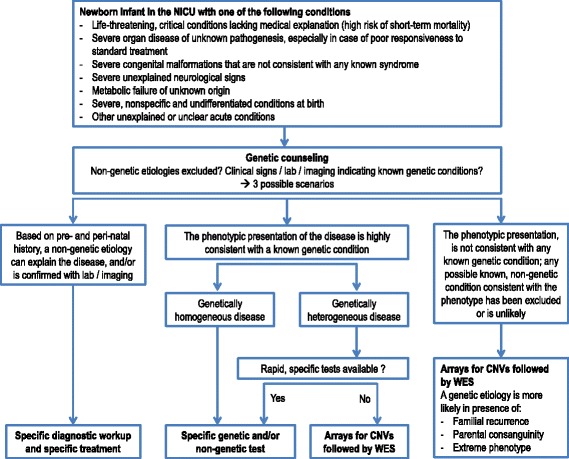
The rapid advancement of next-generation sequencing (NGS) technology and the decrease in costs for whole-exome sequencing (WES) and whole-genome sequening (WGS), has prompted its clinical application in several fields of medicine. Currently, there are no specific guidelines for the use of NGS in the field of neonatal medicine and in the diagnosis of genetic diseases in critically ill newborn infants. As a consequence, NGS may be underused with reduced diagnostic success rate, or overused, with increased costs for the healthcare system. Most genetic diseases may be already expressed during the neonatal age, but their identification may be complicated by nonspecific presentation, especially in the setting of critical clinical conditions. The differential diagnosis process in the neonatal intensive care unit (NICU) may be time-consuming, uncomfortable for the patient due to repeated sampling, and ineffective in reaching a molecular diagnosis during NICU stay. Serial gene sequencing (Sanger sequencing) may be successful only for conditions for which the clinical phenotype strongly suggests a diagnostic hypothesis and for genetically homogeneous diseases. Newborn screenings with Guthrie cards, which vary from country to country, are designed to only test for a few dozen genetic diseases out of the more than 6000 diseases for which a genetic characterization is available. The use of WES in selected cases in the NICU may overcome these issues. We present an intersociety document that aims to define the best indications for the use of WES in different clinical scenarios in the NICU. We propose that WES is used in the NICU for critically ill newborn infants when an early diagnosis is desirable to guide the clinical management during NICU stay, when a strong hypothesis cannot be formulated based on the clinical phenotype or the disease is genetically heterogeneous, and when specific non-genetic laboratory tests are not available. The use of WES may reduce the time for diagnosis in infants during NICU stay and may eventually result in cost-effectiveness.
Keywords: Diagnosis; Genetic; Genome; Mendelian; NICU; Neonatal intensive care unit; Neonate; WES; WGS; Whole-exome sequencing.
Conflict of interest statement
Authors’ information
The respective Scientific Societies of the authors of this paper are as follows: Italian Society of Pediatrics (SIP), Italian Society of Neonatology (SIN), Italian Society of Pediatric Genetic Diseases and Congenital Disabilities (SIMGePed), and Italian Society of Human Genetics (SIGU).
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Tetreault M, Bareke E, Nadaf J, Alirezaie N, Majewski J. Whole-exome sequencing as a diagnostic tool: current challenges and future opportunities. Expert Rev Mol Diagn. 2015;15:749–760. - PubMed
-
- OMIM Gene Map Statistics. http://www.omim.org/statistics/geneMap. Accessed 5 July, 2017.
-
- Saunders CJ, Miller NA, Soden SE, Dinwiddie DL, Noll A, Alnadi NA, Andraws N, Patterson ML, Krivohlavek LA, Fellis J, et al. Rapid whole-genome sequencing for genetic disease diagnosis in neonatal intensive care units. Sci Transl Med. 2012;4:154ra135. doi: 10.1126/scitranslmed.3004041. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
