

Lipidomics reveals accumulation of the oxidized cholesterol in erythrocytes of heart failure patients
- PMID: 29101899
- PMCID: PMC5675899
- DOI: 10.1016/j.redox.2017.10.020
Lipidomics reveals accumulation of the oxidized cholesterol in erythrocytes of heart failure patients
Abstract
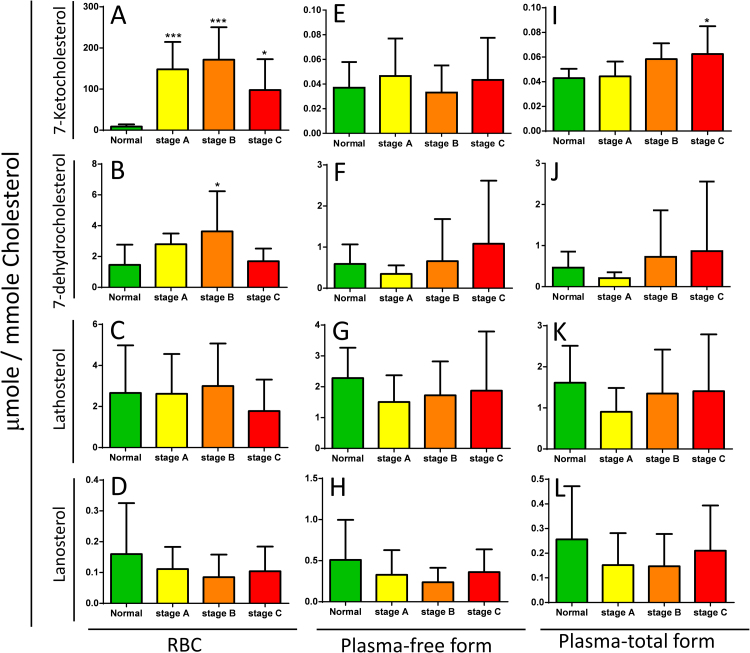
Lipids play an important role in the pathogenesis of cardiovascular disease. Changes in lipids of erythrocytes are indicative of the outcome of pathophysiological processes. In the present study, we assessed whether the lipid profiles of erythrocytes from heart failure (HF) patients are informative of their disease risk. The lipidomes of erythrocytes from 10 control subjects and 29 patients at different HF stages were analyzed using liquid chromatography time-of-flight mass spectrometry. The lipid composition of erythrocytes obtained from HF patients was significantly different from that of normal controls. The levels of phosphatidylcholines (PCs), phosphatidylethanolamines (PEs), and sphingomyelins decreased in HF erythrocytes as compared with those of control subjects; however, the levels of lysoPCs, lysoPEs, and ceramides increased in HF erythrocytes. Notably, the oxidized cholesterol 7-ketocholesterol (7KCh) accumulated to higher level in HF erythrocytes than in plasma from the same patients. We further validated our findings with a cohort of 115 subjects of control subjects (n=28) and patients (n=87). Mechanistically, 7KCh promoted reactive oxygen species (ROS) formation in cardiomyocytes; and induced their death, probably through an ATF4-dependent pathway. Our findings suggest that erythrocytic 7KCh can be a risk factor for HF, and is probably implicated in its pathophysiology.
Keywords: 7-ketocholesterol; Heart failure; Lipidomics; Oxidative stress.
Copyright © 2017 The Authors. Published by Elsevier B.V. All rights reserved.
Figures





References
-
- Bahrami H., Bluemke D.A., Kronmal R. Novel metabolic risk factors for incident heart failure and their relationship with obesity: the MESA (Multi-Ethnic Study of Atherosclerosis) study. J. Am. Coll. Cardiol. 2008;51:1775–1783. - PubMed
-
- Ingelsson E., Arnlov J., Sundstrom J., Zethelius B., Vessby B., Lind L. Novel metabolic risk factors for heart failure. J. Am. Coll. Cardiol. 2005;46:2054–2060. - PubMed
-
- Turer A.T. Using metabolomics to assess myocardial metabolism and energetics in heart failure. J. Mol. Cell Cardiol. 2012 - PubMed
-
- Ingwall J.S. Energetics of the failing heart: new insights using genetic modification in the mouse. Arch. Mal. Coeur Vaiss. 2006;99:839–847. - PubMed
-
- Ashrafian H., Redwood C., Blair E., Watkins H. Hypertrophic cardiomyopathy: a paradigm for myocardial energy depletion. Trends Genet. 2003;19:263–268. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
