

Autonomic Dysfunction in Cardiology: Pathophysiology, Investigation, and Management
- PMID: 29102451
- PMCID: PMC5705288
- DOI: 10.1016/j.cjca.2017.09.008
Autonomic Dysfunction in Cardiology: Pathophysiology, Investigation, and Management
Abstract
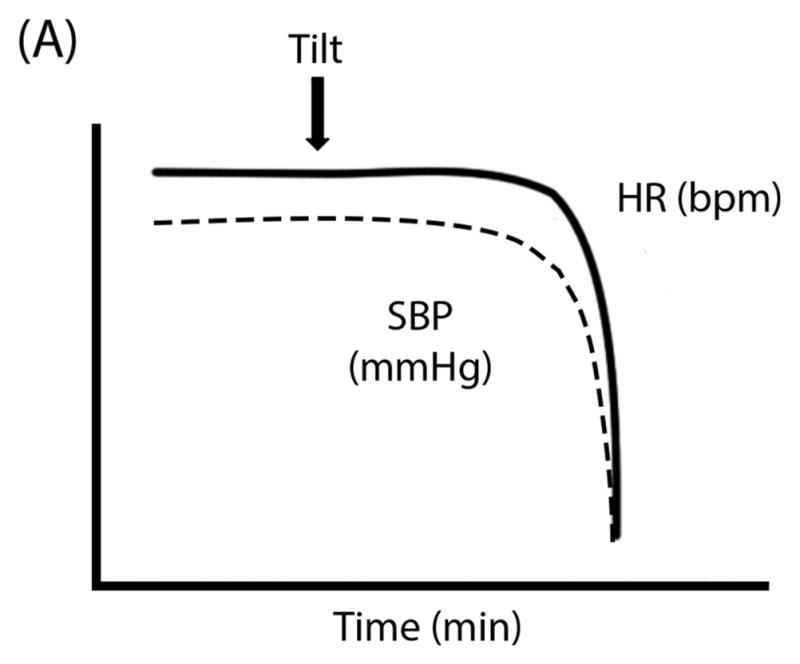
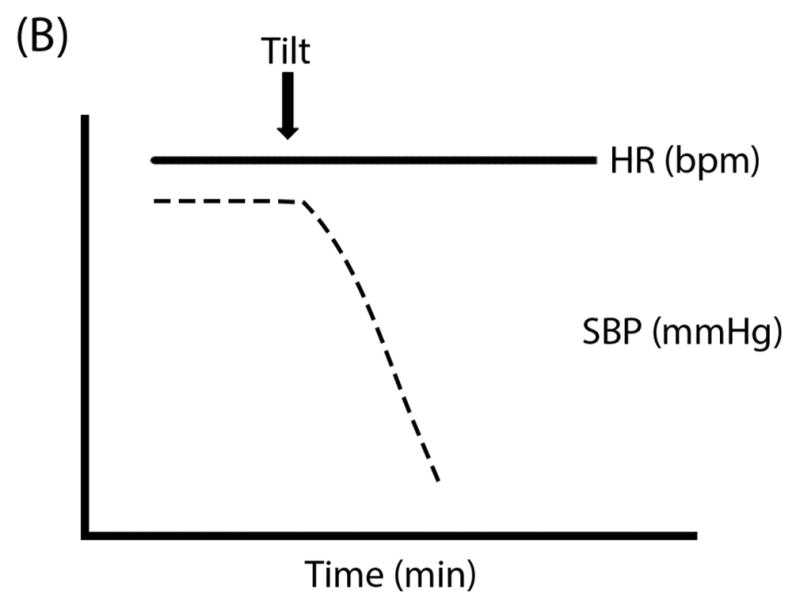
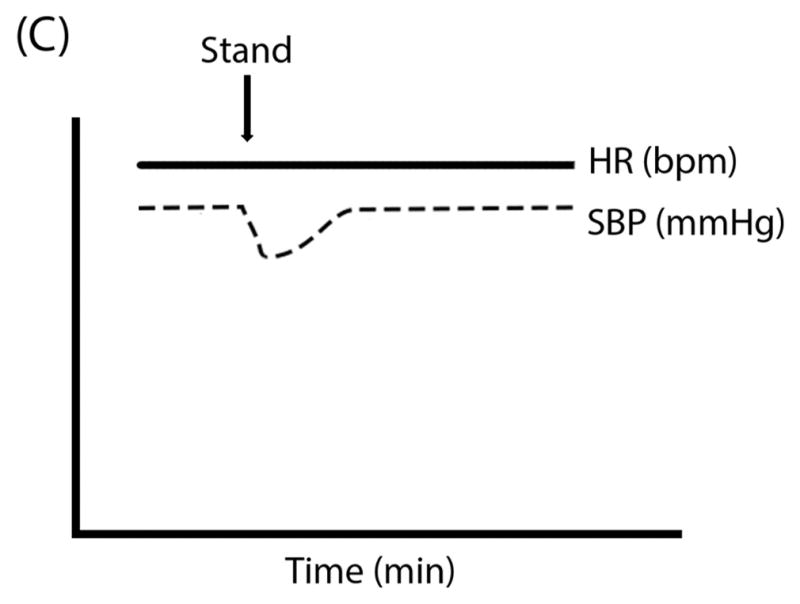
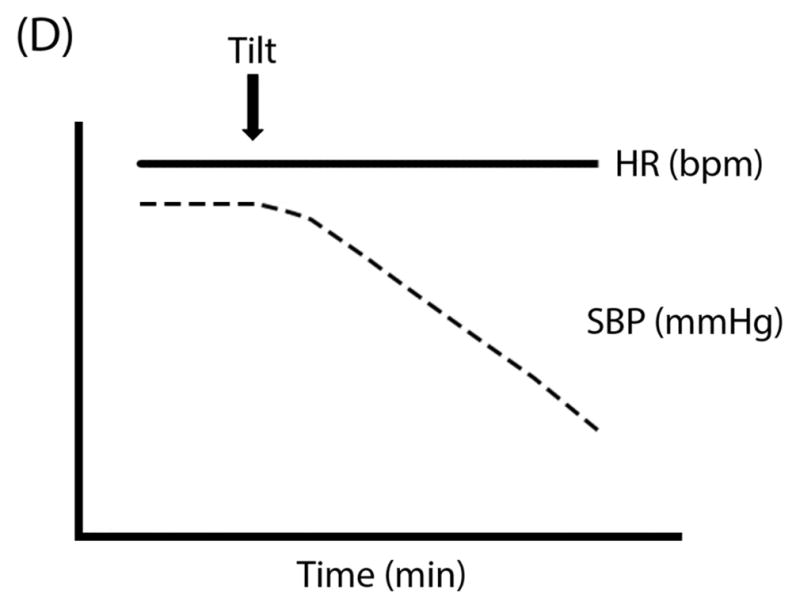
Presyncope and syncope are common medical findings, with a > 40% estimated lifetime prevalence. These conditions are often elicited by postural stress and can be recurrent and accompanied by debilitating symptoms of cerebral hypoperfusion. Therefore, it is critical for physicians to become familiar with the diagnosis and treatment of common underlying causes of presyncope and syncope. In some patients, altered postural hemodynamic responses result from a failure of compensatory autonomic nervous system reflex mechanisms. The most common presentations of presyncope and syncope secondary to this autonomic dysfunction include vasovagal syncope, neurogenic orthostatic hypotension, and postural tachycardia syndrome. The most sensitive method for diagnosis is a detailed initial evaluation with medical history, physical examination, and resting electrocardiogram to rule out cardiac syncope. Physical examination should include measurement of supine and standing blood pressure and heart rate to identify the pattern of hemodynamic regulation during orthostatic stress. Additional testing may be required in patients without a clear diagnosis after the initial evaluation. Management of patients should focus on improving symptoms and functional status and not targeting arbitrary hemodynamic values. An individualized structured and stepwise approach should be taken for treatment, starting with patient education, lifestyle modifications, and use of physical counter-pressure manoeuvres and devices to improve venous return. Pharmacologic interventions should be added only when conservative approaches are insufficient to improve symptoms. There are no gold standard approaches for pharmacologic treatment in these conditions, with medications often used off label and with limited long-term data for effectiveness.
Copyright © 2017 Canadian Cardiovascular Society. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Smith JJ, Porth CM, Erickson M. Hemodynamic response to the upright posture. J Clin Pharmacol. 1994;34:375–386. - PubMed
-
- Chisholm P, Anpalahan M. Orthostatic hypotension: Pathophysiology, assessment, treatment and the paradox of supine hypertension. Intern Med J. 2017;47:370–379. - PubMed
-
- Shen WK, Sheldon RS, Benditt DG, Cohen MI, Forman DE, Goldberger ZD, Grubb BP, Hamdan MH, Krahn AD, Link MS, Olshansky B, Raj SR, Sandhu RK, Sorajja D, Sun BC, Yancy CW. 2017 acc/aha/hrs guideline for the evaluation and management of patients with syncope: Executive summary: A report of the american college of cardiology/american heart association task force on clinical practice guidelines, and the heart rhythm society. J Am Coll Cardiol. 2017 - PubMed
-
- Daccarett M, Jetter TL, Wasmund SL, Brignole M, Hamdan MH. Syncope in the emergency department: Comparison of standardized admission criteria with clinical practice. Europace. 2011;13:1632–1638. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
