

Long-Term Survival Trends of Medicare Patients After In-Hospital Cardiac Arrest: Insights from Get With The Guidelines-Resuscitation®
- PMID: 29102470
- PMCID: PMC5784777
- DOI: 10.1016/j.resuscitation.2017.10.023
Long-Term Survival Trends of Medicare Patients After In-Hospital Cardiac Arrest: Insights from Get With The Guidelines-Resuscitation®
Abstract
Background: Although rates of survival to hospital discharge after in-hospital cardiac arrest (IHCA) have improved over the last decade, it is unknown if these survival gains are sustained after hospital discharge.
Objective: To examine 1-year survival trends overall and by rhythm after IHCA.
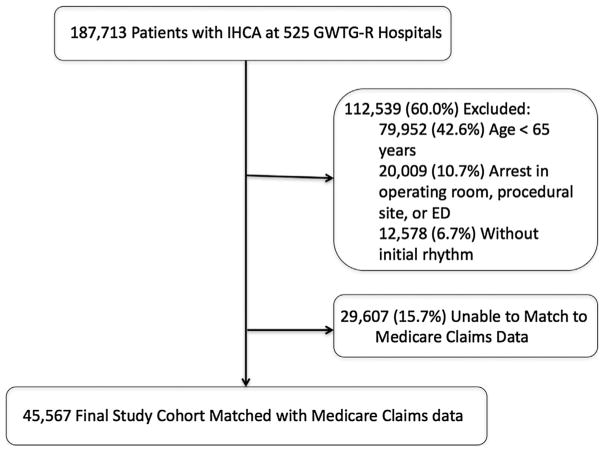
Methods: Using Medicare beneficiaries (age≥65years) with IHCA occurring between 2000 and 2011 at Get With The Guidelines®-Resuscitation Registry participating hospitals we used multivariable regression, to examine temporal trends in risk-adjusted rates of 1-year survival.
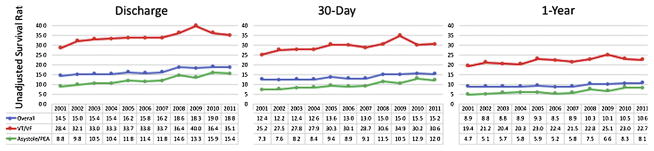
Results: Among 45,567 patients with IHCA, the unadjusted 1-year survival was 9.4%. Unadjusted 1-year survival was 21.8% among the 9,223 (20.2%) of patients with Ventricular Fibrillation or Pulseless Ventricular Tachycardia (VF/VT) and 6.2% among the 36,344 (79.8%) of patients with Pulseless Electrical Activity or asystole (PEA/asystole). After adjustment for patient and arrest characteristics, 1-year survival increased over time for all IHCA from 8.9% in 2000-2001 to 15.2% in 2011 (adjusted rate ratio [RR] per year, 1.05; 95% CI, 1.03-1.06; P<0.001 for trend). Improvements in 1-year risk adjusted survival were also observed for VF/VT (19.4% in 2000-2001 to 25.6% in 2011 [RR per year, 1.02; 95% CI, 1.01-1.04; P 0.004 for trend]) and PEA/asystole arrests (4.7% in 2000-2001 to 10.2% in 2011 [RR per year, 1.07; 95% CI, 1.05-1.08; P<0.001 for trend]).
Conclusion: Among Medicare beneficiaries in the GWTG-Resuscitation registry, 1-year survival after IHCA has increased for over the past decade. Temporal improvements in survival were noted for both shockable and non-shockable presenting arrest rhythms.
Keywords: In-Hospital cardiac arrest; Outcomes; Resuscitation; Survival.
Copyright © 2017 Elsevier B.V. All rights reserved.
Conflict of interest statement
The authors have no relationships with industry to disclose. Dr. Thompson is supported by NIH/NCATS Colorado CTSI Grant Number UL1 TR001082. Dr. Chan is supported by funding from the NIH (1R01HL123980). Dr. Perman is supported by funding from the NIH (K12HD057022). Dr. Daugherty is supported by funding from the NIH (R01HL133343).
Figures
References
-
- Meaney PA, Nadkarni VM, Kern KB, Indik JH, Halperin HR, Berg RA. Rhythms and outcomes of adult in-hospital cardiac arrest. Crit Care Med. 2010;38:101–8. - PubMed
-
- Heffner AC, Pearson DA, Nussbaum ML, Jones AE. Regionalization of post-cardiac arrest care: implementation of a cardiac resuscitation center. Am Heart J. 2012;164:493–501. e2. - PubMed
-
- Peberdy MA, Kaye W, Ornato JP, et al. Cardiopulmonary resuscitation of adults in the hospital: a report of 14720 cardiac arrests from the National Registry of Cardiopulmonary Resuscitation. Resuscitation. 2003;58:297–308. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
