

Familial co-occurrence of congenital heart defects follows distinct patterns
- PMID: 29106500
- PMCID: PMC6018923
- DOI: 10.1093/eurheartj/ehx314
Familial co-occurrence of congenital heart defects follows distinct patterns
Abstract
Aims: Congenital heart defects (CHD) affect almost 1% of all live born children and the number of adults with CHD is increasing. In families where CHD has occurred previously, estimates of recurrence risk, and the type of recurring malformation are important for counselling and clinical decision-making, but the recurrence patterns in families are poorly understood. We aimed to determine recurrence patterns, by investigating the co-occurrences of CHD in 1163 families with known malformations, comprising 3080 individuals with clinically confirmed diagnosis.
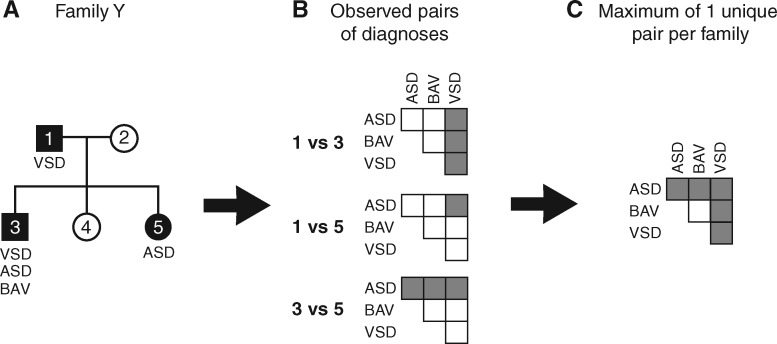
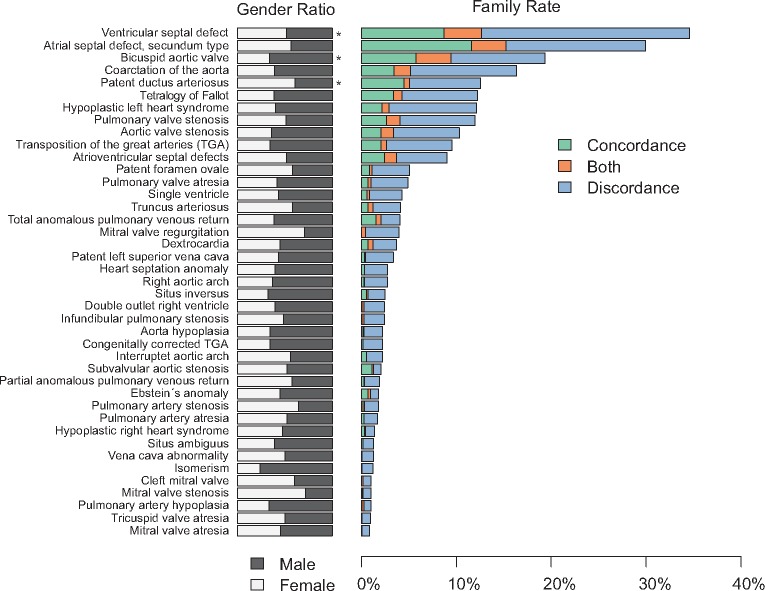
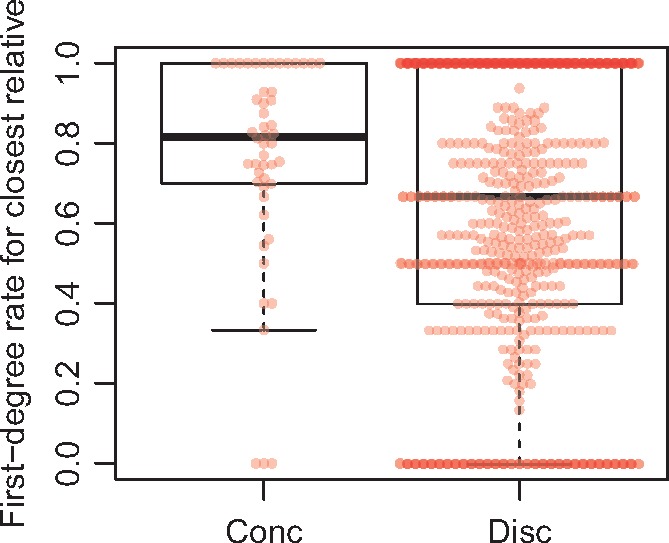
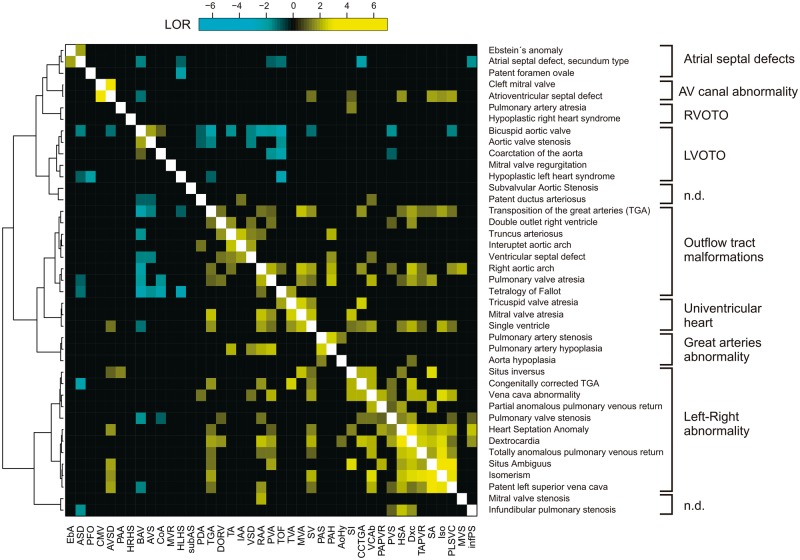
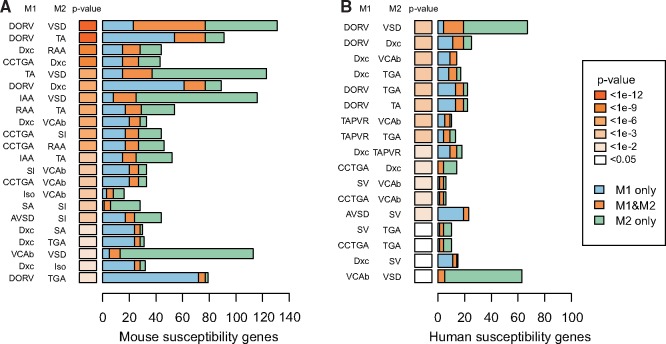
Methods and results: We calculated rates of concordance and discordance for 41 specific types of malformations, observing a high variability in the rates of concordance and discordance. By calculating odds ratios for each of 1640 pairs of discordant lesions observed between affected family members, we were able to identify 178 pairs of malformations that co-occurred significantly more or less often than expected in families. The data show that distinct groups of cardiac malformations co-occur in families, suggesting influence from underlying developmental mechanisms. Analysis of human and mouse susceptibility genes showed that they were shared in 19% and 20% of pairs of co-occurring discordant malformations, respectively, but none of malformations that rarely co-occur, suggesting that a significant proportion of co-occurring lesions in families is caused by overlapping susceptibility genes.
Conclusion: Familial CHD follow specific patterns of recurrence, suggesting a strong influence from genetically regulated developmental mechanisms. Co-occurrence of malformations in families is caused by shared susceptibility genes.
Figures
Comment in
-
A family of diseases in families of patients.Eur Heart J. 2018 Mar 21;39(12):1023-1027. doi: 10.1093/eurheartj/ehx404. Eur Heart J. 2018. PMID: 29020349 No abstract available.
References
-
- Ferencz C, Rubin JD, McCarter RJ, Brenner JI, Neill CA, Perry LW, Hepner SI, Downing JW.. Congenital heart disease: prevalence at livebirth. The Baltimore-Washington Infant Study. Am J Epidemiol 1985;121:31–36. - PubMed
-
- Baumgartner H, Bonhoeffer P, De Groot NM, de HF, Deanfield JE, Galie N, Gatzoulis MA, Gohlke-Baerwolf C, Kaemmerer H, Kilner P, Meijboom F, Mulder BJ, Oechslin E, Oliver JM, Serraf A, Szatmari A, Thaulow E, Vouhe PR, Walma E.. ESC Guidelines for the management of grown-up congenital heart disease (new version 2010). Eur Heart J 2010;31:2915–2957. - PubMed
-
- Gill HK, Splitt M, Sharland GK, Simpson JM.. Patterns of recurrence of congenital heart disease: an analysis of 6,640 consecutive pregnancies evaluated by detailed fetal echocardiography. J Am Coll Cardiol 2003;42:923–929. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
