

Hypothalamic-pituitary-adrenal (HPA) axis suppression after treatment with glucocorticoid therapy for childhood acute lymphoblastic leukaemia
- PMID: 29106702
- PMCID: PMC6486149
- DOI: 10.1002/14651858.CD008727.pub4
Hypothalamic-pituitary-adrenal (HPA) axis suppression after treatment with glucocorticoid therapy for childhood acute lymphoblastic leukaemia
Abstract
Background: Glucocorticoids play a major role in the treatment of acute lymphoblastic leukaemia (ALL). However, supraphysiological doses can suppress the hypothalamic-pituitary-adrenal (HPA) axis. HPA axis suppression resulting in reduced cortisol response may cause an impaired stress response and an inadequate host defence against infection, which remain a cause of morbidity and death. Suppression commonly occurs in the first days after cessation of glucocorticoid therapy, but the exact duration is unclear. This review is the second update of a previously published Cochrane review.
Objectives: To examine the occurrence and duration of HPA axis suppression after (each cycle of) glucocorticoid therapy for childhood ALL.
Search methods: We searched the Cochrane Central Register of Controlled Trials (CENTRAL; 2016, Issue 11), MEDLINE/PubMed (from 1945 to December 2016), and Embase/Ovid (from 1980 to December 2016). In addition, we searched reference lists of relevant articles, conference proceedings (the International Society for Paediatric Oncology and the American Society of Clinical Oncology from 2005 up to and including 2016, and the American Society of Pediatric Hematology/Oncology from 2014 up to and including 2016), and ongoing trial databases (the International Standard Registered Clinical/Social Study Number (ISRCTN) register via http://www.controlled-trials.com, the National Institutes of Health (NIH) register via www.clinicaltrials.gov, and the International Clinical Trials Registry Platform (ICTRP) of the World Health Organization (WHO) via apps.who.int/trialsearch) on 27 December 2016.
Selection criteria: All study designs, except case reports and patient series with fewer than 10 children, examining effects of glucocorticoid therapy for childhood ALL on HPA axis function.
Data collection and analysis: Two review authors independently performed study selection. One review author extracted data and assessed 'Risk of bias'; another review author checked this information.
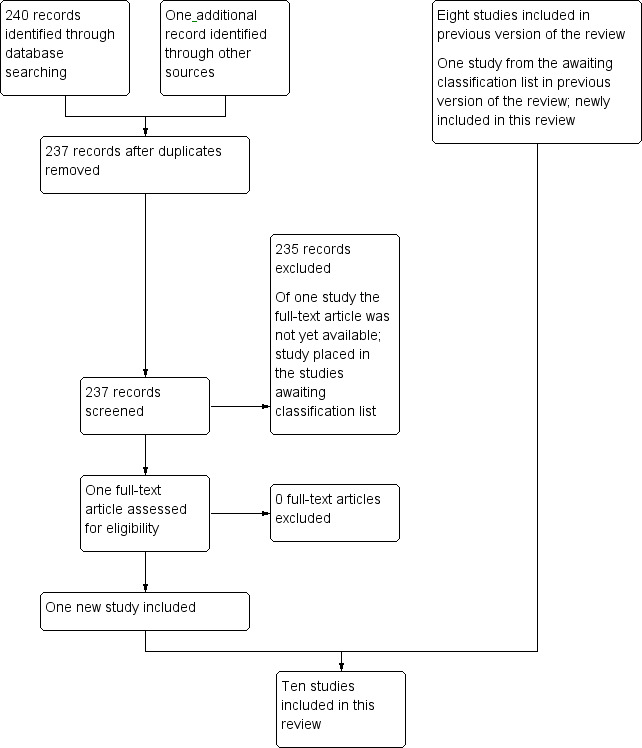
Main results: We identified 10 studies (total of 298 children; we identified two studies for this update) including two randomised controlled trials (RCTs) that assessed adrenal function. None of the included studies assessed the HPA axis at the level of the hypothalamus, the pituitary, or both. Owing to substantial differences between studies, we could not pool results. All studies had risk of bias issues. Included studies demonstrated that adrenal insufficiency occurs in nearly all children during the first days after cessation of glucocorticoid treatment for childhood ALL. Most children recovered within a few weeks, but a small number of children had ongoing adrenal insufficiency lasting up to 34 weeks.Included studies evaluated several risk factors for (prolonged) adrenal insufficiency. First, three studies including two RCTs investigated the difference between prednisone and dexamethasone in terms of occurrence and duration of adrenal insufficiency. The RCTs found no differences between prednisone and dexamethasone arms. In the other (observational) study, children who received prednisone recovered earlier than children who received dexamethasone. Second, treatment with fluconazole appeared to prolong the duration of adrenal insufficiency, which was evaluated in two studies. One of these studies reported that the effect was present only when children received fluconazole at a dose higher than 10 mg/kg/d. Finally, two studies evaluated the presence of infection, stress episodes, or both, as a risk factor for adrenal insufficiency. In one of these studies (an RCT), trial authors found no relationship between the presence of infection/stress and adrenal insufficiency. The other study found that increased infection was associated with prolonged duration of adrenal insufficiency.
Authors' conclusions: We concluded that adrenal insufficiency commonly occurs in the first days after cessation of glucocorticoid therapy for childhood ALL, but the exact duration is unclear. No data were available on the levels of the hypothalamus and the pituitary; therefore, we could draw no conclusions regarding these outcomes. Clinicians may consider prescribing glucocorticoid replacement therapy during periods of serious stress in the first weeks after cessation of glucocorticoid therapy for childhood ALL to reduce the risk of life-threatening complications. However, additional high-quality research is needed to inform evidence-based guidelines for glucocorticoid replacement therapy.Special attention should be paid to patients receiving fluconazole therapy, and perhaps similar antifungal drugs, as these treatments may prolong the duration of adrenal insufficiency, especially when administered at a dose higher than 10 mg/kg/d.Finally, it would be relevant to investigate further the relationship between present infection/stress and adrenal insufficiency in a larger, separate study specially designed for this purpose.
Conflict of interest statement
None.
Update of
-
Hypothalamic-pituitary-adrenal (HPA) axis suppression after treatment with glucocorticoid therapy for childhood acute lymphoblastic leukaemia.Cochrane Database Syst Rev. 2015 Aug 17;(8):CD008727. doi: 10.1002/14651858.CD008727.pub3. Cochrane Database Syst Rev. 2015. Update in: Cochrane Database Syst Rev. 2017 Nov 06;11:CD008727. doi: 10.1002/14651858.CD008727.pub4. PMID: 26282194 Updated.
References
References to studies included in this review
Cunha 2004 {published and unpublished data}
-
- Cunha CF, Silva IN, Finch FL. Early adrenocortical recovery after glucocorticoid therapy in children with leukemia. Journal of Clinical Endocrinology and Metabolism 2004;89(6):2797‐802. - PubMed
Einaudi 2008 {published and unpublished data}
-
- Einaudi S, Bertorello N, Masera N, Farinasso L, Barisone E, Rizzari C, et al. Adrenal axis function after high‐dose steroid therapy for childhood acute lymphoblastic leukemia. Pediatric Blood & Cancer 2008;50(3):537‐41. - PubMed
Felner 2000 {published and unpublished data}
-
- Felner EI, Thompson MT, Ratliff AF, White PC, Dickson BA. Time course of recovery of adrenal function in children treated for leukemia. Journal of Pediatrics 2000;137(1):21‐4. - PubMed
Kuperman 2001 {published data only (unpublished sought but not used)}
-
- Kuperman H, Damiani D, Chrousos GP, Dichtchekenian V, Manna TD, Filho VO, et al. Evaluation of the hypothalamic‐pituitary‐adrenal axis in children with leukemia before and after 6 weeks of high‐dose glucocorticoid therapy. Journal of Clinical Endocrinology & Metabolism 2001;86(7):2993‐6. - PubMed
Kuperman 2012 {published and unpublished data}
-
- Kuperman H, Filho VO, Cristofani LM, Assis de Almeida MT, Setian N, Damiani D. Evaluation of adrenal reserve in children with acute lymphoblastic leukemia treated with prednisone or dexamethasone. Hormone Research in Paediatrics 2012;78:73‐80. - PubMed
Mahachoklertwattana 2004 {published and unpublished data}
-
- Mahachoklertwattana P, Vilaiyuk S, Hongeng S, Okascharoen C. Suppression of adrenal function in children with acute lymphoblastic leukemia following induction therapy with corticosteroid and other cytotoxic agents. Journal of Pediatrics 2004;144(6):736‐40. - PubMed
Perdomo‐Ramírez 2016 {published and unpublished data}
-
- Perdomo‐Ramírez I, Linares‐Ballesteros A, Acevedo‐Sedano L, Coll‐Barrios M. Hypothalamus‐pituitary‐adrenal axis suppression following induction chemotherapy in children with acute lymphoblastic leukemia [Supresión del eje hipotálamo‐hipófisis‐suprarrenal después de la quimioterapia de inducción en niños con leucemia linfoide aguda]. Iatreia 2016;29(1):18‐26.
Petersen 2003 {published and unpublished data}
-
- Petersen KB, Müller J, Rasmussen M, Schmiegelow K. Impaired adrenal function after glucocorticoid therapy in children with acute lymphoblastic leukemia. Medical and Pediatric Oncology 2003;41(2):110‐4. - PubMed
Rix 2005 {published and unpublished data}
-
- Rix M, Birkebaek NH, Rosthøj S, Clausen N. Clinical impact of corticosteroid‐induced adrenal suppression during treatment for acute lymphoblastic leukemia in children: a prospective observational study using the low‐dose adrenocorticotropin test. Journal of Pediatrics 2005;147(5):645‐50. - PubMed
Salem 2015 {published and unpublished data}
-
- Salem A, Tantawy A, Sedfy H, Laboudy M, Toaima D, Mahmoud N, et al. A prospective study of the hypothalamic‐pituitary‐adrenal axis in children with acute lymphoblastic leukemia receiving chemotherapy. Hematology 2015;20(6):320‐7. - PubMed
References to studies excluded from this review
Bessho 1984 {published data only}
-
- Bessho F, Kagawa J, Mizutani S, Egi S, Fujiu M, Kaku H, et al. Effects of antileukemic therapy of endocrine functions and development of children. European Paediatric Haematology and Oncology 1984;1:135‐41.
Birkebaek 1998 {published data only (unpublished sought but not used)}
-
- Birkebaek NH, Fisker S, Clausen N, Tuovinen V, Sindet‐Pedersen S, Christiansen JS. Growth and endocrinological disorders up to 21 years after treatment for acute lymphoblastic leukemia in childhood. Medical and Pediatric Oncology 1998;30(6):351‐6. - PubMed
Felder‐Puig 2007 {published data only}
-
- Felder‐Puig R, Scherzer C, Baumgartner M, Ortner M, Aschenbrenner C, Bieglmayer C, et al. Glucocorticoids in the treatment of children with acute lymphoblastic leukemia and Hodgkin's disease: a pilot study on the adverse psychological reactions and possible associations with neurobiological, endocrine, and genetic markers. Clinical Cancer Research 2007;13(23):7093‐100. - PubMed
Felner 2011 {published data only}
-
- Felner EL. Reducing the risk for adrenal insufficiency in those treated for all: tapering glucocorticoids before abrupt discontinuation. Journal of Pediatric Hematology/Oncology 2011;33:406‐8. - PubMed
Lightner 1981 {published data only}
-
- Lightner ES, Johnson H, Corrigan JJ Jr. Rapid adrenocortical recovery after short‐term glucocorticoid therapy. American Journal of Diseases of Children 1981;135(9):790‐2. - PubMed
Pawlaczyk 1993 {published data only}
-
- Pawlaczyk B, Malecka EH, Krause W. Adrenocortical function and reserve in children treated for acute lymphoblastic leukaemia [Czynnosc i rezerwa korowo‐nadnerczowa u dzieci po leczeniu ostrej bialaczki limfoblastycznej]. Pediatria Polska 1993;68:49‐54.
Silva 2006 {published data only}
-
- Silva IN, Cunha CF, Finch FL, Colosimo EA. Evaluation of hypothalamic‐pituitary‐adrenal axis recovery after corticotherapy by using basal cortisol secretion [Avaliação da recuperação do eixo hipotalâmicohipofisário‐adrenal após corticoterapia por meio do cortisol basal]. Arquivos Brasileiros de Endocrinologia e Metabologia 2006;50(1):118‐24. - PubMed
Vestergaard 2011 {published data only}
-
- Vestergaard TR, Anders J, Lausten‐Thomsen U, Lausen B, Hjalgrim H, Kvist TK, et al. Duration of adrenal insufficiency during treatment for childhood acute lymphoblastic leukemia. Journal of Pediatric Hematology/Oncology 2011;33:442‐9. - PubMed
References to studies awaiting assessment
Schlosser 2016 {published and unpublished data}
-
- Schlosser M, Burd D, Ahmet A, Lawrence S, Bassal M. Adrenal suppression in pediatric patients during maintenance treatment for acute lymphoblastic leukemia. Pediatric Blood and Cancer 2016;63(Suppl S1 (29th Annual Meeting of the American Society of Pediatric Hematology/Oncology (ASPHO), 11‐14 May, Minneapolis, MN, USA)):S41.
Additional references
Abdu 1999
-
- Abdu TA, Elhadd TA, Neary R, Clayton RN. Comparison of the low dose short synacthen test (1 microg), the conventional dose short synacthen test (250 microg), and the insulin tolerance test for assessment of the hypothalamo‐pituitary‐adrenal axis in patients with pituitary disease. Journal of Clinical Endocrinology and Metabolism 1999;84(3):838‐43. - PubMed
Agwu 1999
Albert 2001
-
- Albert SG, DeLeon MJ, Silverberg AB. Possible association between high‐dose fluconazole and adrenal insufficiency in critically ill patients. Critical Care Medicine 2001;29(3):668‐70. - PubMed
Biostat, Inc, USA
-
- Borenstein M, Rothstein H. Comprehensive Meta Analysis. Comprehensive Meta‐Analysis. Englewood, New Jersey, USA: Biostat, Inc. , 1999.
Böttner 2005
-
- Böttner A, Kratzsch J, Liebermann S, Keller A, Pfaffle RW, Kiess W, et al. Comparison of adrenal function tests in children ‐ the glucagon stimulation test allows the simultaneous assessment of adrenal function and growth hormone response in children. Journal of Pediatric Endocrinology & Metabolism 2005;18(5):433‐42. - PubMed
Christensen 2005
-
- Christensen MS, Heyman M, Möttönen M, Zeller B, Jonmundsson G, Hasle H. Treatment‐related death in childhood acute lymphoblastic leukaemia in the Nordic countries: 1992‐2001. British Journal of Haematology 2005;131(1):50‐8. - PubMed
DCOG 2014
-
- DCOG. Leukemia [Leukemie]. https://www.skion.nl/voor‐patienten‐en‐ouders/ziektebeelden/542/ziektebe... 2014 (accessed June 2014).
Dickstein 1997
-
- Dickstein G, Spigel D, Arad E, Shechner C. One microgram is the lowest ACTH dose to cause a maximal cortisol response. There is no diurnal variation of cortisol response to submaximal ACTH stimulation. European Journal of Endocrinology 1997;137(2):172‐5. - PubMed
Grimes 2002
-
- Grimes DA, Schulz KF. Cohort studies: marching towards outcomes. The Lancet 2002;359(9303):341‐5. - PubMed
Henzen 2000
-
- Henzen C, Suter A, Lerch E, Urbinelli R, Schorno XH, Briner VA. Suppression and recovery of adrenal response after short‐term, high‐dose glucocorticoid treatment. The Lancet 2000;85(2):542‐5. - PubMed
Hettmannsperger 1992
-
- Hettmannsperger U, Detmar M, Owskianowski M, Tenorio S, Kammler HJ, Orfanos CE. Cytokine‐stimulated human dermal microvascular endothelial cells produce interleukin 6 ‐ inhibition by hydrocortisone, dexamethasone, and calcitriol. Journal of Investigative Dermatology 1992;99(5):531‐6. - PubMed
Higgins 2011
-
- Higgins JPT, Green S (editors). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. www.handbook.cochrane.org.
Hurwitz 2000
-
- Hurwitz CA, Silverman LB, Schorin MA, Clavell LA, Dalton VK, Glick KM, et al. Substituting dexamethasone for prednisone complicates remission induction in children with acute lymphoblastic leukemia. Cancer 2000;88(8):1964‐9. - PubMed
Igarashi 2005
-
- Igarashi S, Manabe A, Ohara A, Kumagai M, Saito T, Okimoto Y, et al. No advantage of dexamethasone over prednisolone for the outcome of standard‐ and intermediate‐risk childhood acute lymphoblastic leukemia in the Tokyo Children's Cancer Study Group L95‐14 protocol. American Journal of Clinical Oncology 2005;23(27):6489‐98. - PubMed
Krasner 1999
-
- Krasner AS. Glucocorticoid‐induced adrenal insufficiency. JAMA 1999;282(7):671‐6. - PubMed
Laupacis 1994
-
- Laupacis A, Wells G, Richardson WS, Tugwell P. Users' guides to the medical literature. V. How to use an article about prognosis. Evidence‐Based Medicine Working Group. JAMA 1994;272(3):234‐7. - PubMed
Leclercq 2013
-
- Leclercq E, Leeflang MMG, Dalen EC, Kremer LCM. Validation of search filters for identifying pediatric studies in PubMed. Journal of Pediatrics 2013;162:629‐34. - PubMed
Maghnie 2005
-
- Maghnie M, Uga E, Temporini F, lorgi N, Secco A, Tinelli C, et al. Evaluation of adrenal function in patients with growth hormone deficiency and hypothalamic‐pituitary disorders: comparison between insulin‐induced hypoglycemia, low‐dose ACTH and CRH stimulation tests. European Journal of Endocrinology 2005;152(5):735‐41. - PubMed
Module CCG
-
- Kremer LCM, Leclercq E, Noorman JK, Jellema P, Dalen EC. Cochrane Childhood Cancer Group. About The Cochrane Collaboration (Cochrane Review Groups (CRGs)) 2017, issue 4:Art. No.: CHILDCA.
Nyhlén 2000
-
- Nyhlén K, Linden M, Andersson R, Uppugunduri S. Corticosteroids and interferons inhibit cytokine‐induced production of IL‐8 by human endothelial cells. Cytokine 2000;12(4):355‐60. - PubMed
Planey 2000
-
- Planey SL, Litwack G. Glucocorticoid‐induced apoptosis in lymphocytes. Biochemical and Biophysical Research Communications 2000;279(2):307‐12. - PubMed
Pruckner 2009
-
- Pruckner C, Attarbaschi A, Peters C, Dworzak MN, Pötschger U, Urban C, et al. Induction death and treatment‐related mortality in first remission of children with acute lymphoblastic leukemia: a population‐based analysis of the Austrian Berlin‐Frankfurt‐Münster study group. Leukemia 2009;23(7):1264‐9. - PubMed
Rao 1987
-
- Rao RH, Spathis GS. Intramuscular glucagon as a provocative stimulus for the assessment of pituitary function: growth hormone and cortisol responses. Metabolism 1987;36(7):658‐63. - PubMed
Rubnitz 2004
-
- Rubnitz JE, Lensing S, Zhou Y, Sandlund JT, Razzouk BI, Ribeiro RC. Death during induction therapy and first remission of acute leukemia in childhood: the St. Jude experience. Cancer 2004;101(7):1677‐84. - PubMed
Schlaghecke 1992
-
- Schlaghecke R, Kornely E, Santen RT, Ridderskamp P. The effect of long‐term glucocorticoid therapy on pituitary‐adrenal responses to exogenous corticotropin‐releasing hormone. New England Journal of Medicine 1992;326(4):226‐30. - PubMed
Shah 1992
Shibata 2001
-
- Shibata S, Kami M, Kanda Y, Machida U, Iwata H, Kishi Y, et al. Acute adrenal failure associated with fluconazole after administration of high‐dose cyclophosphamide. American Journal of Hematology 2001;66(4):303‐5. - PubMed
Shulman 2007
-
- Shulman DI, Palmert MR, Kemp SF, Lawson Wilkins Drug and Therapeutics Committee. Adrenal insufficiency: still a cause of morbidity and death in childhood. Pediatrics 2007;119(2):484‐94. - PubMed
Te Poele 2007
-
- Poele EM, Bont ES, Marike Boezen H, Revesz T, Bökkerink JP, Bieshuizen A, et al. Dexamethasone in the maintenance phase of acute lymphoblastic leukaemia treatment: is the risk of lethal infections too high?. European Journal of Cancer 2007;43(17):2532‐6. - PubMed
Tordjman 2000
-
- Tordjman K, Jaffe A, Trostanetsky Y, Greenman Y, Limor R, Stern N. Low‐dose (1 microgram) adrenocorticotrophin (ACTH) stimulation as a screening test for impaired hypothalamo‐pituitary‐adrenal axis function: sensitivity, specificity and accuracy in comparison with the high‐dose (250 microgram) test. Clinical Endocrinology 2000;52(5):633‐40. - PubMed
Van Tijn 2008
-
- Tijn DA, Vijlder JJ, Vulsma T. Role of corticotropin‐releasing hormone testing in assessment of hypothalamic‐pituitary‐adrenal axis function in infants with congenital central hypothyroidism. Journal of Clinical Endocrinology & Metabolism 2008;93(10):3794‐803. - PubMed
Vanderschueren‐Lodeweyckx 1974
-
- Vanderschueren‐Lodeweyckx M, Wolter R, Malvaux P, Eggermont E, Eeckels R. The glucagon stimulation test: effect of plasma growth hormone and on immunoreactive insulin, cortisol, and glucose in children. Journal of Pediatrics 1974;85(2):182‐7. - PubMed
Waage 1988
References to other published versions of this review
Gordijn 2010
-
- Gordijn MS, Gemke RJBJ, Dalen EC, Rotteveel J, Kaspers GJL. Hypothalamic‐pituitary‐adrenal (HPA) axis suppression after treatment with glucocorticoid therapy for childhood acute lymphoblastic leukemia. Cochrane Database of Systematic Reviews 2010, Issue 10. [DOI: 10.1002/14651858.CD008727] - DOI - PMC - PubMed
Gordijn 2012
-
- Gordijn MS, Gemke RJBJ, Dalen EC, Rotteveel J, Kaspers GJL. Hypothalamic‐pituitary‐adrenal (HPA) axis suppression after treatment with glucocorticoid therapy for childhood acute lymphoblastic leukaemia. Cochrane Database of Systematic Reviews 2012, Issue 5. [DOI: 10.1002/14651858.CD008727.pub2] - DOI - PubMed
Gordijn 2015
-
- Gordijn MS, Rensen N, Gemke RJBJ, Dalen EC, Rotteveel J, Kaspers GJL. Hypothalamic‐pituitary‐adrenal (HPA) axis suppression after treatment with glucocorticoid therapy for childhood acute lymphoblastic leukaemia. Cochrane Database of Systematic Reviews 2015, Issue 8. [DOI: 10.1002/14651858.CD008727.pub3] - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical