

Optimal threshold of controlled attenuation parameter with MRI-PDFF as the gold standard for the detection of hepatic steatosis
- PMID: 29108123
- PMCID: PMC5867216
- DOI: 10.1002/hep.29639
Optimal threshold of controlled attenuation parameter with MRI-PDFF as the gold standard for the detection of hepatic steatosis
Abstract
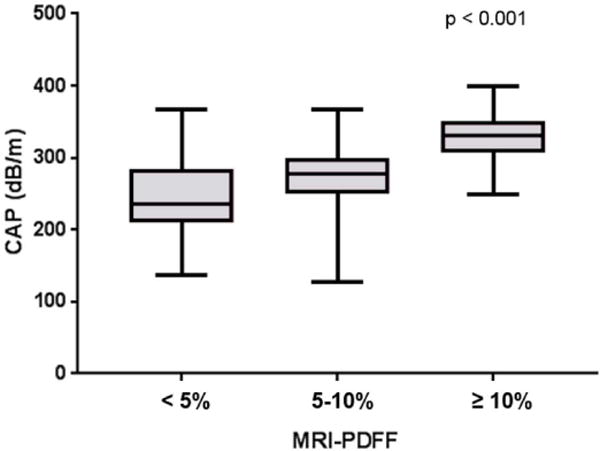
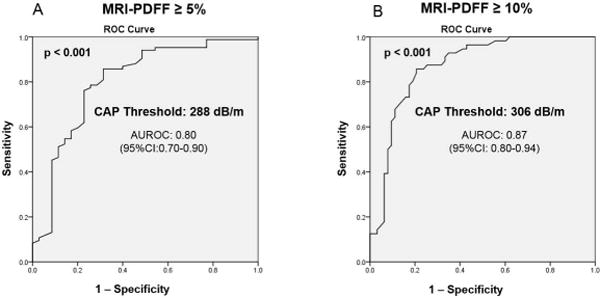
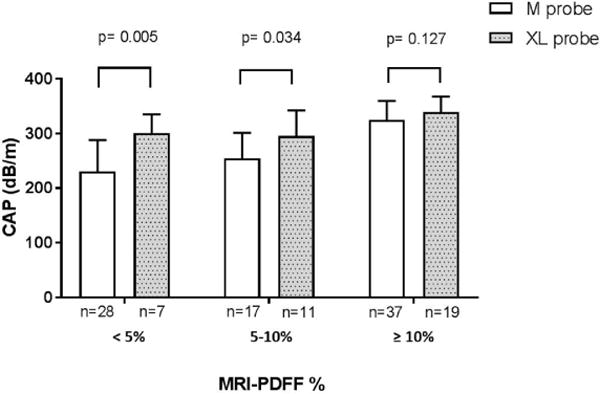
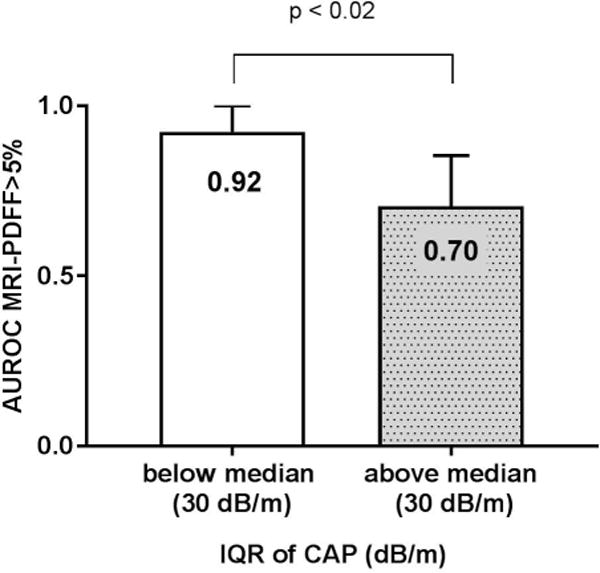
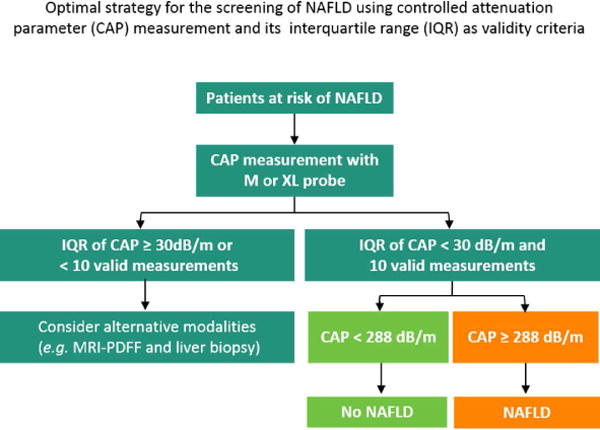
The optimal threshold of controlled attenuation parameter (CAP) for the detection of hepatic steatosis using both M and XL probe is unknown in nonalcoholic fatty liver disease (NAFLD). Magnetic resonance imaging proton density fat fraction (MRI-PDFF) is an accurate and precise method of detecting the presence of hepatic steatosis that is superior to CAP. Thus, the aim of this study was to evaluate the diagnostic accuracy and optimal threshold of CAP for the detection of hepatic steatosis as defined by MRI-PDFF ≥ 5%. This prospective cross-sectional study included 119 adults (59% women) with and without NAFLD who underwent MRI-PDFF and CAP using either M or XL probe when indicated within a 6-month period at the NAFLD Research Center, University of California, San Diego. The mean ( ± standard deviation) age and body mass index were 52.4 (±15.2) years and 29.9 (±5.5) kg/m2 , respectively. The prevalence of NAFLD (MRI-PDFF ≥ 5%) and MRI-PDFF ≥ 10% was 70.6% and 47.1%, respectively. The area under the receiver operating characteristic (AUROC) of CAP for the detection of MRI-PDFF ≥ 5% was 0.80 (95% confidence interval [CI], 0.70-0.90) at the cut-point of 288 dB/m and of MRI-PDFF ≥ 10% was 0.87 (95% CI, 0.80-0.94) at the cut-point of 306 dB/m. When stratified by the interquartile range (IQR) of CAP, we observed that an IQR below the median (30 dB/m) had a robust AUROC compared with an IQR above the median (0.92 [95% CI, 0.85-1.00] versus 0.70 [95% CI, 0.56-0.85]; P = 0.0117), and these differences were statistically and clinically significant.
Conclusion: The cut-point of CAP for presence of hepatic steatosis (MRI-PDFF ≥ 5%) was 288 dB/m. The diagnostic accuracy of CAP for the detection of hepatic steatosis is more reliable when the IQR of CAP is <30 dB/m. These data have implications for the clinical use of CAP in the assessment of NAFLD. (Hepatology 2018;67:1348-1359).
© 2017 by the American Association for the Study of Liver Diseases.
Conflict of interest statement
Figures
References
-
- Younossi ZM, Koenig AB, Abdelatif D, Fazel Y, Henry L, Wymer M. Global epidemiology of nonalcoholic fatty liver disease-Meta-analytic assessment of prevalence, incidence, and outcomes. Hepatology. 2016;64:73–84. - PubMed
-
- Loomba R, Sanyal AJ. The global NAFLD epidemic. Nat Rev Gastroenterol Hepatol. 2013;10:686–690. - PubMed
-
- Williams CD, Stengel J, Asike MI, Torres DM, Shaw J, Contreras M, Landt CL, et al. Prevalence of nonalcoholic fatty liver disease and nonalcoholic steatohepatitis among a largely middle-aged population utilizing ultrasound and liver biopsy: a prospective study. Gastroenterology. 2011;140:124–131. - PubMed
-
- Fazel Y, Koenig AB, Sayiner M, Goodman ZD, Younossi ZM. Epidemiology and natural history of non-alcoholic fatty liver disease. Metabolism. 2016;65:1017–1025. - PubMed
-
- Charlton MR, Burns JM, Pedersen RA, Watt KD, Heimbach JK, Dierkhising RA. Frequency and outcomes of liver transplantation for nonalcoholic steatohepatitis in the United States. Gastroenterology. 2011;141:1249–1253. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
