

Associations of Salivary BPIFA1 Protein in Chronic Periodontitis Patients with Type 2 Diabetes Mellitus
- PMID: 29109737
- PMCID: PMC5646319
- DOI: 10.1155/2017/1087017
Associations of Salivary BPIFA1 Protein in Chronic Periodontitis Patients with Type 2 Diabetes Mellitus
Abstract
Aims: To explore the differences in salivary BPI fold containing family A, member 1 (BPIFA1) concentration among type 2 diabetes mellitus (T2DM) subjects with various severities of chronic periodontitis and to determine whether BPIFA1 in saliva can be used as a potential biomarker of T2DM.
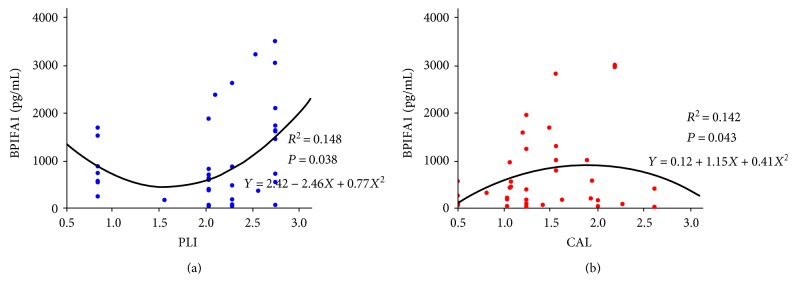
Methods: Unstimulated saliva samples were collected from 44 subjects with T2DM and 44 without T2DM (NDM). Additionally, demographic data and general health parameters, including fasting blood glucose (FBG) and body mass index (BMI), were collected. We also detected full-mouth clinical periodontal parameters including probing pocket depth (PPD), clinical attachment level (CAL), bleeding index (BI), and plaque index (PLI). Salivary BPIFA1, tumor necrosis factor-α (TNF-α), and interleukin-6 (IL-6) concentrations were also detected.
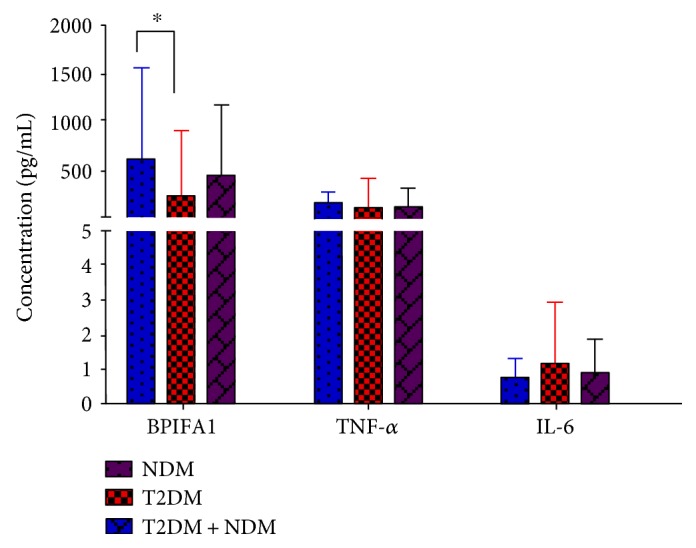
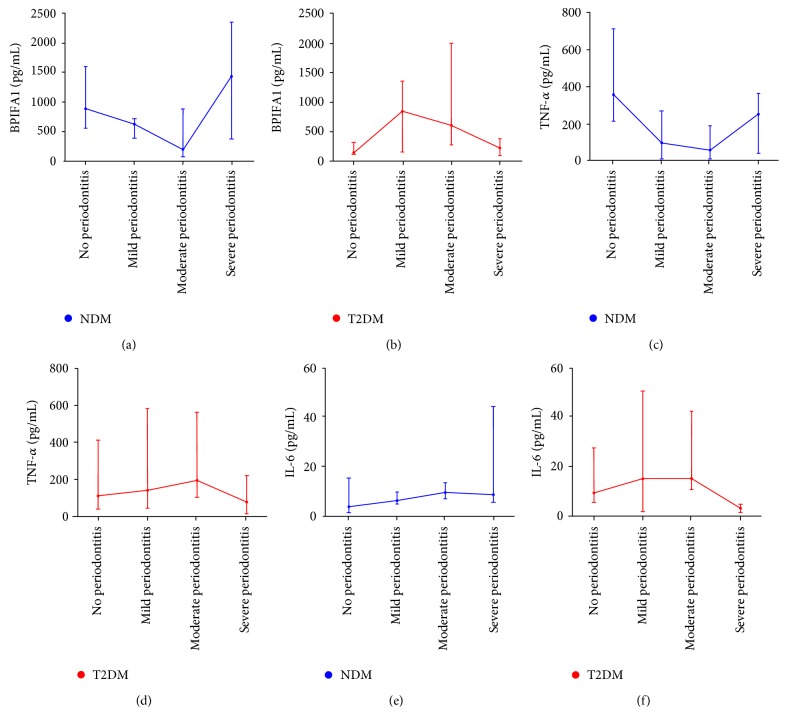
Results: BPIFA1 in saliva was detected at relatively high levels. T2DM subjects had decreased salivary BPIFA1 concentrations (P = 0.031). In T2DM subjects with nonperiodontitis or severe periodontitis, the level of BPIFA1 was significantly lower compared with that of NDM. Salivary TNF-α concentration displayed a similar trend to BPIFA1 in the NDM group.
Conclusions: BPIFA1 protein is rich in saliva and might be used as a potential predictive biomarker of T2DM, especially in patients with severe periodontitis and nonperiodontitis. This trial is registered with ChiCTR-ROC-17010310.
Figures
Similar articles
-
Salivary interleukin-17 and tumor necrosis factor-α in relation to periodontitis and glycemic status in type 2 diabetes mellitus.J Diabetes. 2015 Sep;7(5):681-8. doi: 10.1111/1753-0407.12228. Epub 2014 Dec 23. J Diabetes. 2015. PMID: 25327309
-
Serum and salivary ferritin and Hepcidin levels in patients with chronic periodontitis and type 2 diabetes mellitus.BMC Oral Health. 2018 Apr 10;18(1):63. doi: 10.1186/s12903-018-0524-4. BMC Oral Health. 2018. PMID: 29636044 Free PMC article.
-
Does metabolic control affect salivary adipokines in type 2 diabetes mellitus?Dent Med Probl. 2019 Jan-Mar;56(1):11-20. doi: 10.17219/dmp/103417. Dent Med Probl. 2019. PMID: 30951617
-
Effects of statins on cytokines levels in gingival crevicular fluid and saliva and on clinical periodontal parameters of middle-aged and elderly patients with type 2 diabetes mellitus.PLoS One. 2021 Jan 8;16(1):e0244806. doi: 10.1371/journal.pone.0244806. eCollection 2021. PLoS One. 2021. PMID: 33417619 Free PMC article.
-
Differential Association of Salivary Proinflammatory Mediators with Type 2 Diabetes: A Network Meta-Analysis.Iran J Public Health. 2024 Dec;53(12):2613-2624. Iran J Public Health. 2024. PMID: 39759198 Free PMC article. Review.
Cited by
-
Impact of the Glycemic Level on the Salivary Proteome of Middle-Aged and Elderly People With Type 2 Diabetes Mellitus: An Observational Study.Front Mol Biosci. 2021 Dec 10;8:790091. doi: 10.3389/fmolb.2021.790091. eCollection 2021. Front Mol Biosci. 2021. PMID: 34957219 Free PMC article.
-
Advanced glycosylated end products restrain the osteogenic differentiation of the periodontal ligament stem cell.J Dent Sci. 2019 Jun;14(2):146-151. doi: 10.1016/j.jds.2019.03.007. Epub 2019 Apr 16. J Dent Sci. 2019. PMID: 31210888 Free PMC article.
References
-
- Shlomo Melmed K. S. P., Larsen P. R., Kronenberg H. M. Williams Textbook of Endocrinology. 2011.
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
