

Lipoxin A4 improves erectile dysfunction in rats with type I diabetes by inhibiting oxidative stress and corporal fibrosis
- PMID: 29111541
- PMCID: PMC5858102
- DOI: 10.4103/aja.aja_49_17
Lipoxin A4 improves erectile dysfunction in rats with type I diabetes by inhibiting oxidative stress and corporal fibrosis
Abstract
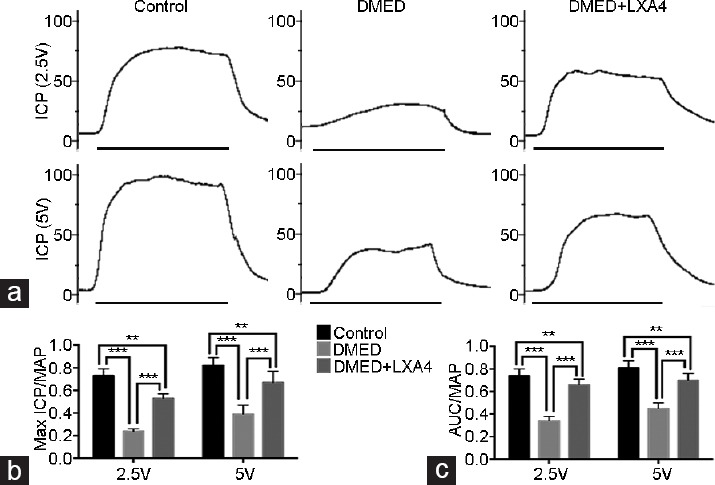
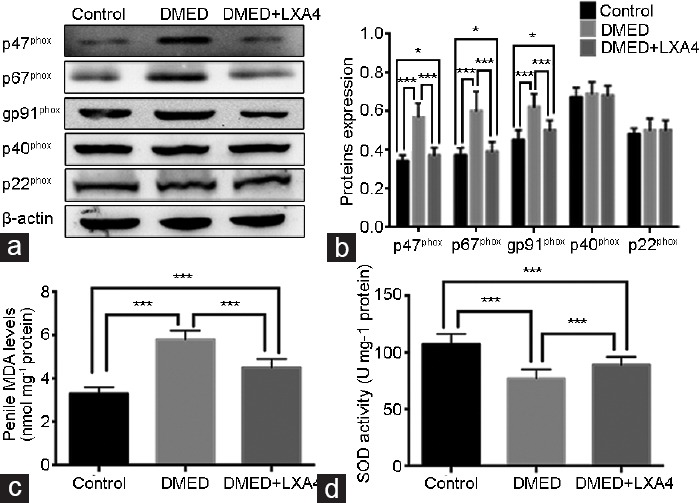
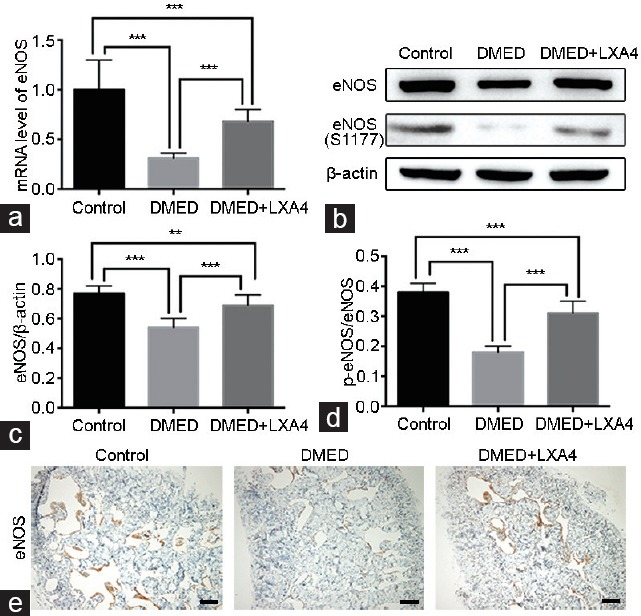
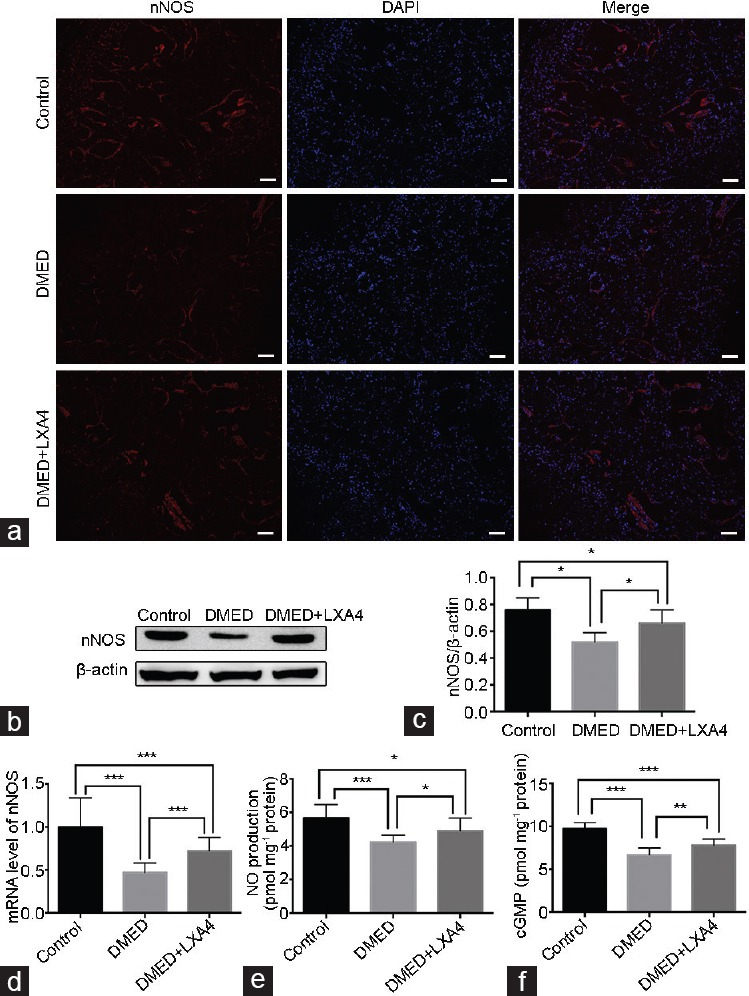
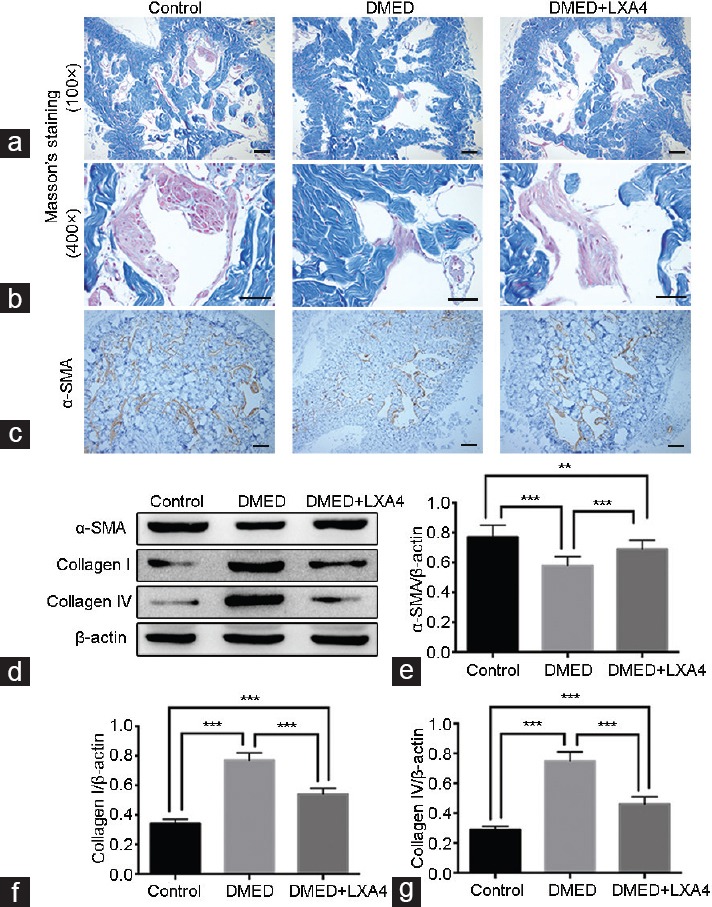
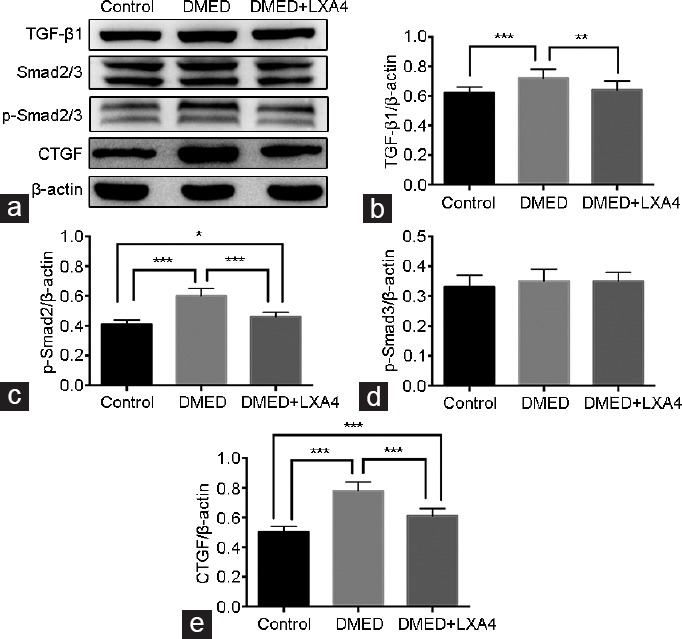
Previous studies have shown that oxidative stress and corporal fibrosis in penile tissues of rats were key pathological factors of erectile dysfunction induced by diabetic mellitus (DMED). Lipoxin A4 (LXA4) was reported to inhibit oxidative stress and fibrosis diseases, while whether it could exert a protective role on erectile function was not clear. Type I diabetic mellitus (DM) was induced in thirty male 10-week-old Sprague-Dawley rats using streptozotocin. Ten weeks later, twenty-two rats with DMED confirmed by an apomorphine test were divided into two groups: the DMED group (n = 11) and the DMED + LXA4 group (n = 11; LXA4 injection daily for 4 weeks). In addition, another ten age-matched rats formed the Control group. We found that erectile function was significantly impaired in the DMED group compared with the Control group, but was improved in the DMED + LXA4 group. Similarly, the over-activated oxidative stress and impaired endothelial function in the DMED group were both improved in the DMED + LXA4 group. Moreover, the DMED group showed serious corporal fibrosis, which was also inhibited by the treatment of LXA4 in the DMED + LXA4 group. Taken together, LXA4 could exert an inhibition role on oxidative stress and fibrosis to improve DMED effectively.
Keywords: diabetic mellitus; erectile dysfunction; fibrosis; oxidative stress.
Figures
References
-
- Shamloul R, Ghanem H. Erectile dysfunction. Lancet. 2013;381:153–65. - PubMed
-
- Shiri R, Koskimaki J, Hakkinen J, Tammela TL, Huhtala H, et al. Effects of age, comorbidity and lifestyle factors on erectile function: Tampere Ageing Male Urological Study (TAMUS) Eur Urol. 2004;45:628–33. - PubMed
-
- Feldman HA, Goldstein I, Hatzichristou DG, Krane RJ, McKinlay JB. Impotence and its medical and psychosocial correlates: results of the Massachusetts Male Aging Study. J Urol. 1994;151:54–61. - PubMed
-
- Johannes CB, Araujo AB, Feldman HA, Derby CA, Kleinman KP, et al. Incidence of erectile dysfunction in men 40 to 69 years old: longitudinal results from the Massachusetts Male Aging Study. J Urol. 2000;163:460–3. - PubMed
-
- Andersen I, Heitmann BL, Wagner G. Obesity and sexual dysfunction in younger Danish men. J Sex Med. 2008;5:2053–60. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
