

Predictive Factors for Long Operative Duration in Patients Undergoing Laparoscopic Cholecystectomy After Endoscopic Retrograde Cholangiography for Combined Choledochocystolithiasis
- PMID: 29112097
- PMCID: PMC5732633
- DOI: 10.1097/SLE.0000000000000461
Predictive Factors for Long Operative Duration in Patients Undergoing Laparoscopic Cholecystectomy After Endoscopic Retrograde Cholangiography for Combined Choledochocystolithiasis
Abstract
Purpose: Choledochocystolithiasis and its associated complications such as cholangitis and pancreatitis are managed by endoscopic retrograde cholangiography (ERC), with endoscopic stone extraction followed by laparoscopic cholecystectomy (LC). However, affected patients present with complex conditions linked to operative difficulties in performing LC. The aim of this study was to elucidate the predictive factors for a prolonged LC procedure following ERC for treating patients with choledochocystolithiasis.
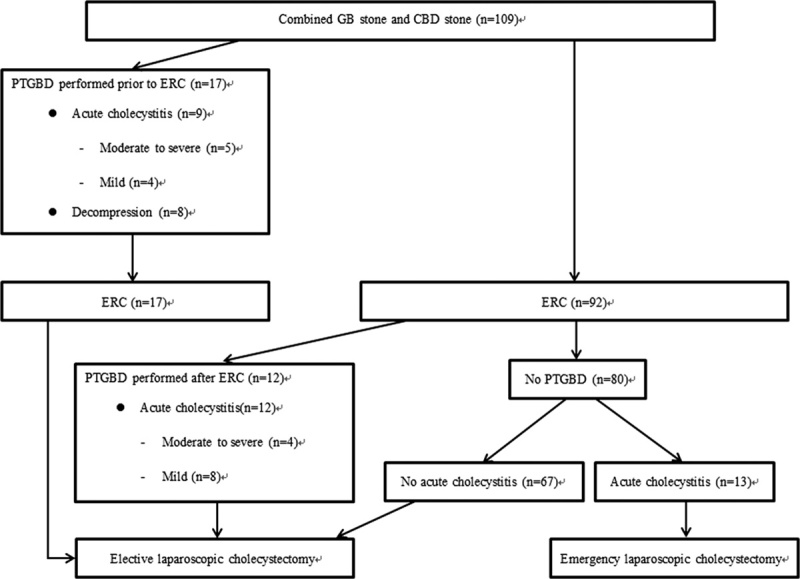
Materials and methods: The medical records of 109 patients who underwent LC after ERC for choledochocystolithiasis from September 2012 to August 2014 were evaluated retrospectively. The cases were divided into long and short operative duration groups using a cutoff operative time of 90 minutes. We used univariate and multivariate analyses to investigate predictive factors associated with long operative duration according to clinical variables, ERC-related factors, and peak serum levels of laboratory test values between the initial presentation and LC (intervening period).
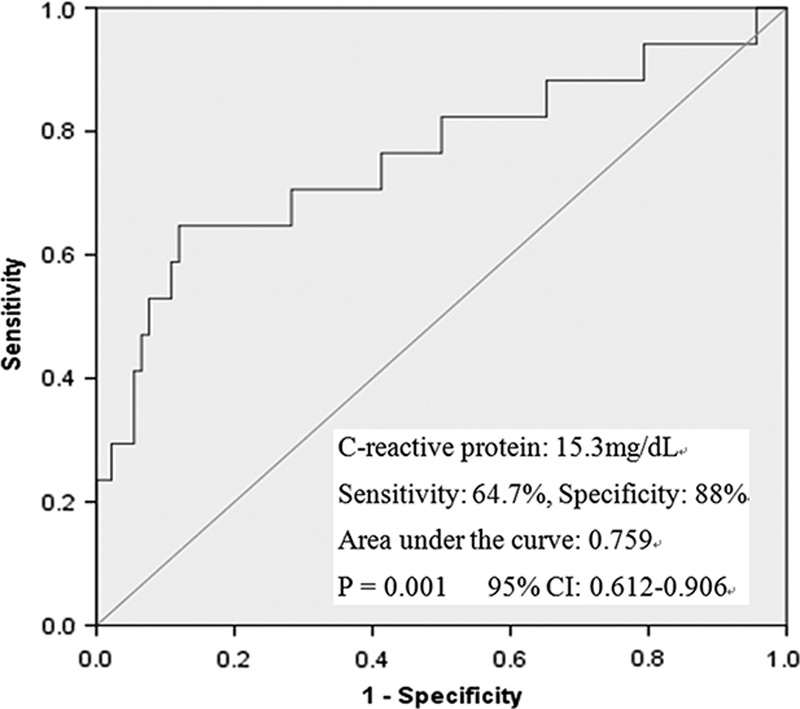
Results: Seventeen patients needed >90 min to complete LC. The presence of acute cholecystitis, placement of percutaneous transhepatic gallbladder drainage, higher peak serum white blood cell count and levels of C-reactive protein (CRP), and lower peak serum levels of lipase during the intervening period were associated with prolonged operative duration. Multivariate analysis showed that the independent predictive factors for long operative duration were the presence of acute cholecystitis (hazard ratio, 5.418; P=0.016) and higher peak levels of CRP (hazard ratio, 1.077; P=0.022).
Conclusion: When patients with choledochocystolithiasis are scheduled for LC after ERC, the presence of acute cholecystitis and high CRP levels during the intervening period could predict a protracted operation.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
-
- Baucom RB, Feurer ID, Shelton JS, et al. Surgeons, ERCP, and laparoscopic common bile duct exploration: do we need a standard approach for common bile duct stones? Surg Endosc. 2016;30:414–423. - PubMed
-
- Ann KS, Kim YH, Kang KJ, et al. Impact of preoperative ERCP on laparoscopic cholecystectomy: a case-controlled study with propensity score matching. World J Surg. 2015;39:2235–2242. - PubMed
-
- Ishizaki Y, Miwa K, Yoshinmoto J, et al. Conversion of elective laparoscopic cholecystectomy to open cholecystectomy between 1993 and 2004. Br J Surg. 2006;93:987–991. - PubMed
-
- Saad WEA, Wallace MJ, Wojak J, et al. Quality improvement guidelines for percutaneous transhepatic cholangiography, biliary drainage, and percutaneous cholecystostomy. J Vasc Interv Radiol. 2010;21:789–795. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
