

Baroreflex Sensitivity and Blood Pressure Variability can Help in Understanding the Different Response to Therapy During Acute Phase of Septic Shock
- PMID: 29112634
- PMCID: PMC5991174
- DOI: 10.1097/SHK.0000000000001046
Baroreflex Sensitivity and Blood Pressure Variability can Help in Understanding the Different Response to Therapy During Acute Phase of Septic Shock
Abstract
Background: Mean values of hemodynamic variables are poorly effective in evaluating an actual recovery of the short-term autonomic mechanisms for blood pressure (BP) and heart rate (HR) regulation. The aim of this work is to analyze the response to therapy in the early phase of septic shock to verify possible associations between BP recovery and BP autonomic control.
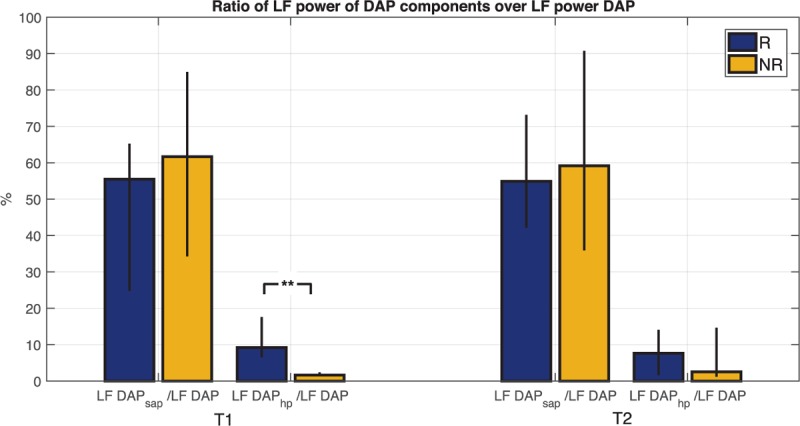
Methods: This is an ancillary study from the multicenter prospective observational trial Shockomics (NCT02141607). A total of 21 septic shock patients were studied at two time points during the acute phase of shock and were classified according to changes in SOFA score. Time series of BP components and HR were analyzed in time and frequency domain. Baroreflex sensitivity (BRS) was assessed, and a mathematical model for the decomposition of diastolic arterial pressure (DAP) oscillations was used to understand the different contributions of BRS and HR on peripheral vascular resistance control.
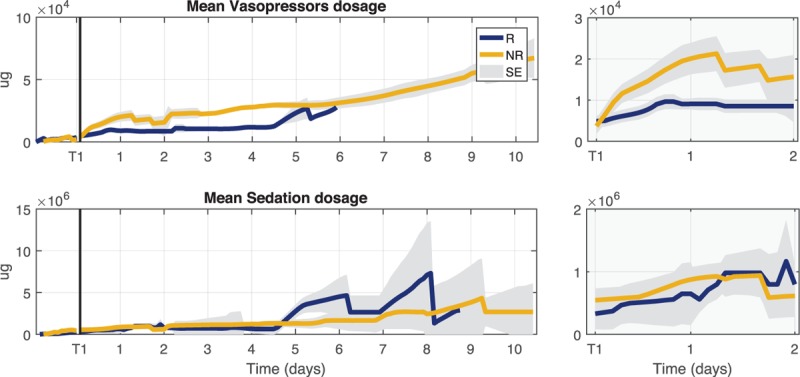
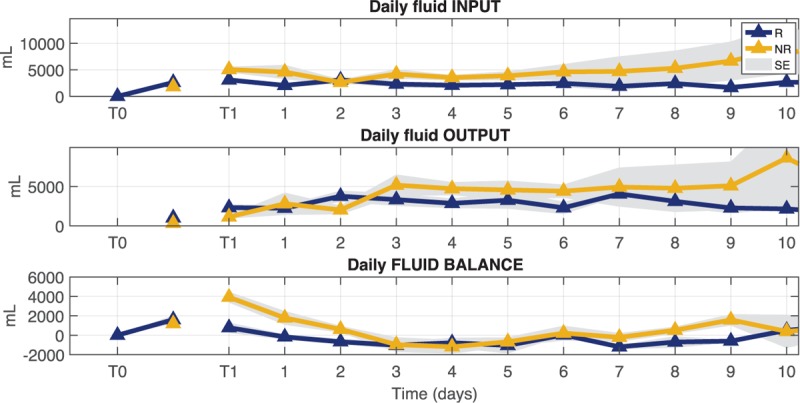
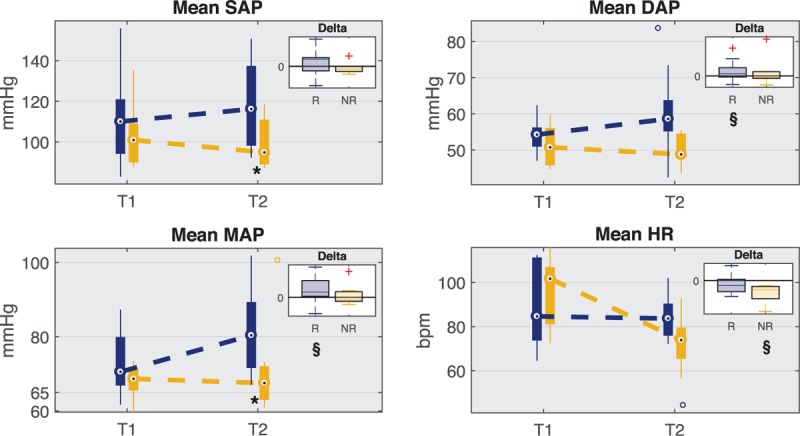
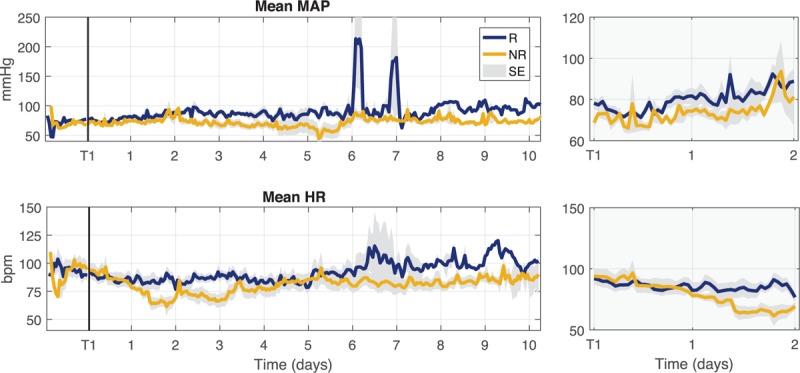
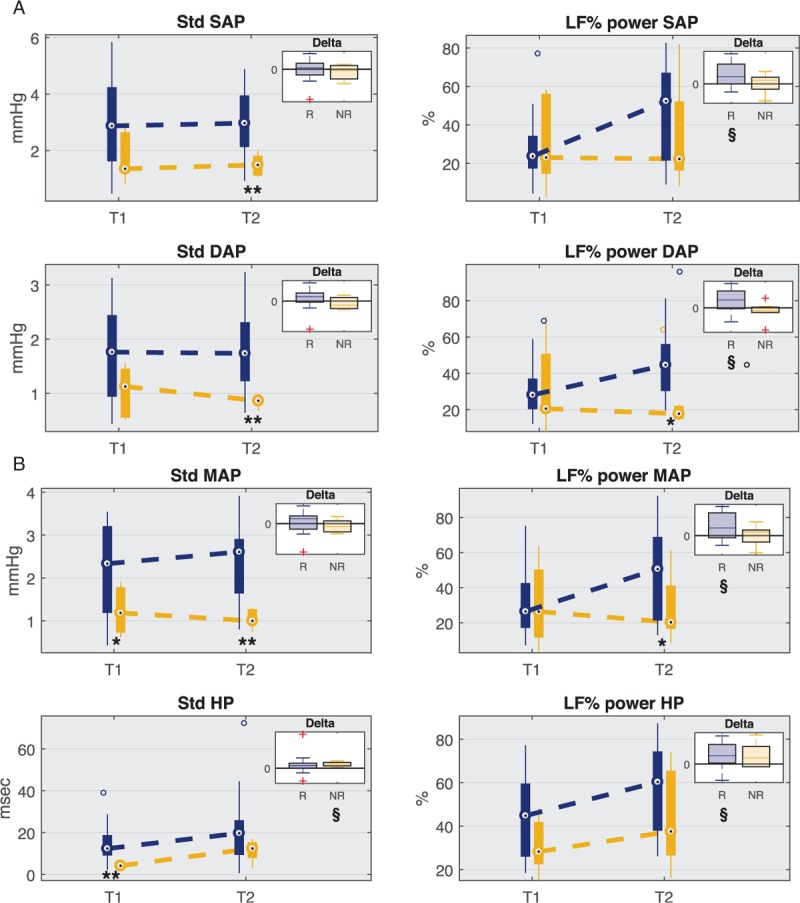
Results: Only those patients, who significantly improved organ function (responders, R), showed an increase of mean value and low frequency (LF) power in BP time series. Fluid accumulation was higher in the non-responders (NR). BRS increased in NR and the model of DAP variability showed that the contribution of HR was highly reduced in NR.
Conclusions: Although patients reached the mean BP target of 65 mmHg, our analyses highlighted important differences in terms of autonomic nervous system control. BP variability, HR variability and baroreflex trends can add information to individual vital sign measure such as mean BP, and can help in understanding the responsiveness to the combination of symphatomimetic drugs and fluid therapy.
Conflict of interest statement
The authors report no conflicts of interest.
Figures
References
-
- Peake SL, Delaney A, Bailey M, Bellomo R, Cameron PA, Cooper DJ, Higgins AM, Holdgate A, et al. ARISE Investigators, ANZICS Clinical Trials Group. Goal-directed resuscitation for patients with early septic shock. N Engl J Med 2014; 371:1496–1506. - PubMed
-
- Mouncey PR, Osborn TM, Power GS, Harrison DA, Sadique MZ, Grieve RD, Jahan R, Harvey SE, Bell D, Bion JF, et al. Trial of early, goal-directed resuscitation for septic shock. N Engl J Med 2015; 372:1301–1311. - PubMed
-
- Kelm DJ, Perrin JT, Cartin-Ceba R, Gajic O, Schenck L, Kennedy CC. Fluid overload in patients with severe sepsis and septic shock treated with early goal-directed therapy is associated with increased acute need for fluid-related medical interventions and hospital death. Shock 2015; 43:68–73. - PMC - PubMed
-
- Rivers E, Nguyen B, Havstad S, Ressler J, Muzzin A, Knoblich B, Peterson E, Tomlanovich M. Early goal-directed therapy in the treatment of severe sepsis and septic shock. N Engl J Med 2001; 345:1368–1377. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
