

Disparities in Chronic Conditions Among Women Hospitalized for Delivery in the United States, 2005-2014
- PMID: 29112666
- PMCID: PMC5709216
- DOI: 10.1097/AOG.0000000000002357
Disparities in Chronic Conditions Among Women Hospitalized for Delivery in the United States, 2005-2014
Abstract
Objective: To estimate trends in the prevalence and socioeconomic distribution of chronic conditions among women hospitalized for obstetric delivery in the United States.
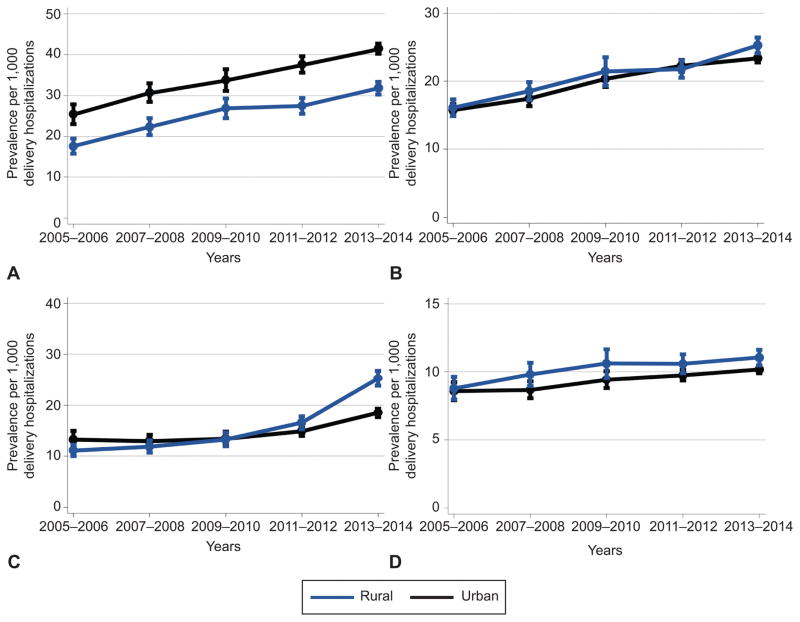
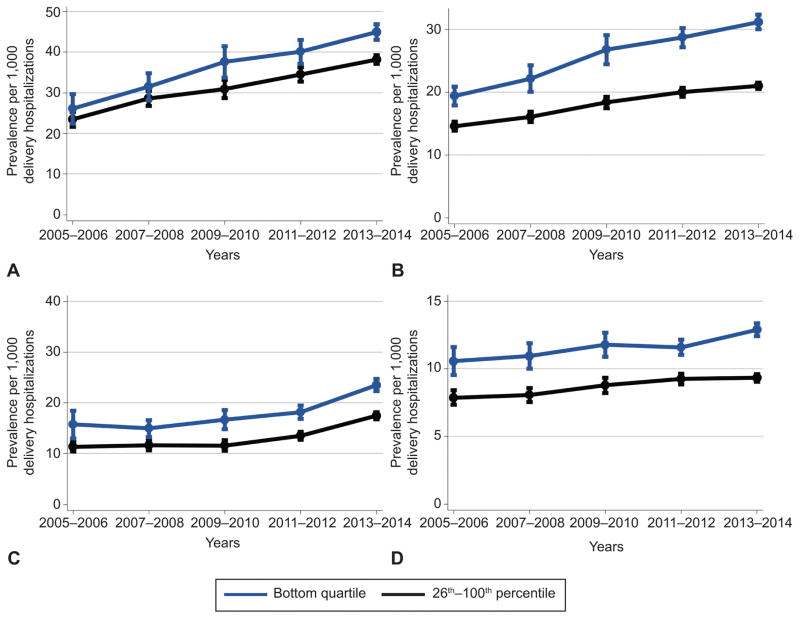
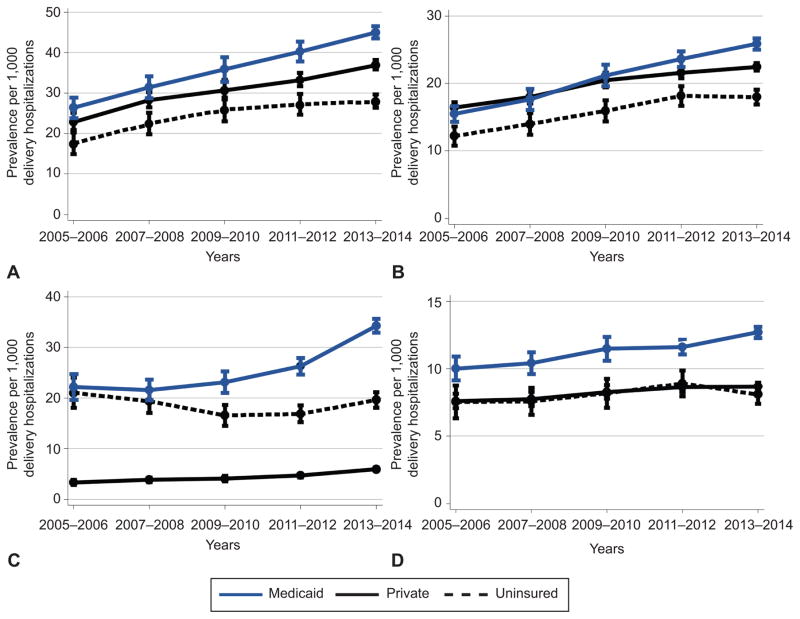
Methods: A retrospective, serial cross-sectional analysis was conducted using 2005-2014 data from the National Inpatient Sample. We estimated the prevalence of eight common, chronic conditions, each associated with obstetric morbidity and mortality, among all childbearing women and then across socioeconomic predictors of obstetric outcomes. Differences over time were measured and compared across rural and urban residence, income, and payer subgroups for each condition.
Results: We identified 8,193,707 delivery hospitalizations, representing 39,273,417 delivery hospitalizations occurring nationally between 2005 and 2014. Identification of at least one chronic condition increased significantly between 2005-2006 and 2013-2014 (66.9 per 1,000 delivery hospitalizations in 2005-2006 compared with 91.8 per 1,000 delivery hospitalizations in 2013-2014). The prevalence of multiple chronic conditions also increased during the study period, from 4.7 (95% CI 4.2-5.2) to 8.1 (95% CI 7.8-8.4) per 1,000 delivery hospitalizations between 2005-2006 and 2013-2014. Chronic respiratory disease, chronic hypertension, substance use disorders, and pre-existing diabetes were the disorders with the greatest increases in prevalence over time. Increasing disparities over time were identified across all socioeconomic subgroups analyzed including rural compared with urban residence, income, and payer. Key areas of concern include the rate at which substance use disorders rose among rural women and the disproportionate burden of each condition among women from the lowest income communities and among women with Medicaid as their primary payer.
Conclusion: Between 2005-2006 and 2013-2014, the prevalence of chronic conditions increased across all segments of the childbearing population. Widening disparities were identified over time with key areas of concern including disproportionate, progressive increases in the burden of chronic conditions among women from rural and low-income communities and those with deliveries funded by Medicaid.
Figures
References
-
- Pregnancy Mortality Surveillance System: Trends in Pregnancy-Related Deaths. Division of Reproductive Health, Centers for Disease Control; Available at: https://www.cdc.gov/reproductivehealth/maternalinfanthealth/pmss.html. Retrieved February 7, 2017.
-
- Mhyre JM, Bateman BT, Leffert LR. Influence of patient comorbidities on the risk of near-miss maternal morbidity or mortality. Anesthesiology. 2011;115:963–72. - PubMed
-
- Creanga AA, Bateman BT, Kuklina EV, Callaghan WM. Racial and ethnic disparities in severe maternal morbidity: a multistate analysis, 2008–2010. Am J Obstet Gynecol. 2014;210:435e1–8. - PubMed
-
- Kuklina EV, Callaghan WM. Chronic heart disease and severe obstetric morbidity among hospitalisations for pregnancy in the USA: 1995–2006. BJOG. 2011;118:345–52. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
