

Contemporary disengagement from antiretroviral therapy in Khayelitsha, South Africa: A cohort study
- PMID: 29112692
- PMCID: PMC5675399
- DOI: 10.1371/journal.pmed.1002407
Contemporary disengagement from antiretroviral therapy in Khayelitsha, South Africa: A cohort study
Abstract
Background: Retention in care is an essential component of meeting the UNAIDS "90-90-90" HIV treatment targets. In Khayelitsha township (population ~500,000) in Cape Town, South Africa, more than 50,000 patients have received antiretroviral therapy (ART) since the inception of this public-sector program in 2001. Disengagement from care remains an important challenge. We sought to determine the incidence of and risk factors associated with disengagement from care during 2013-2014 and outcomes for those who disengaged.
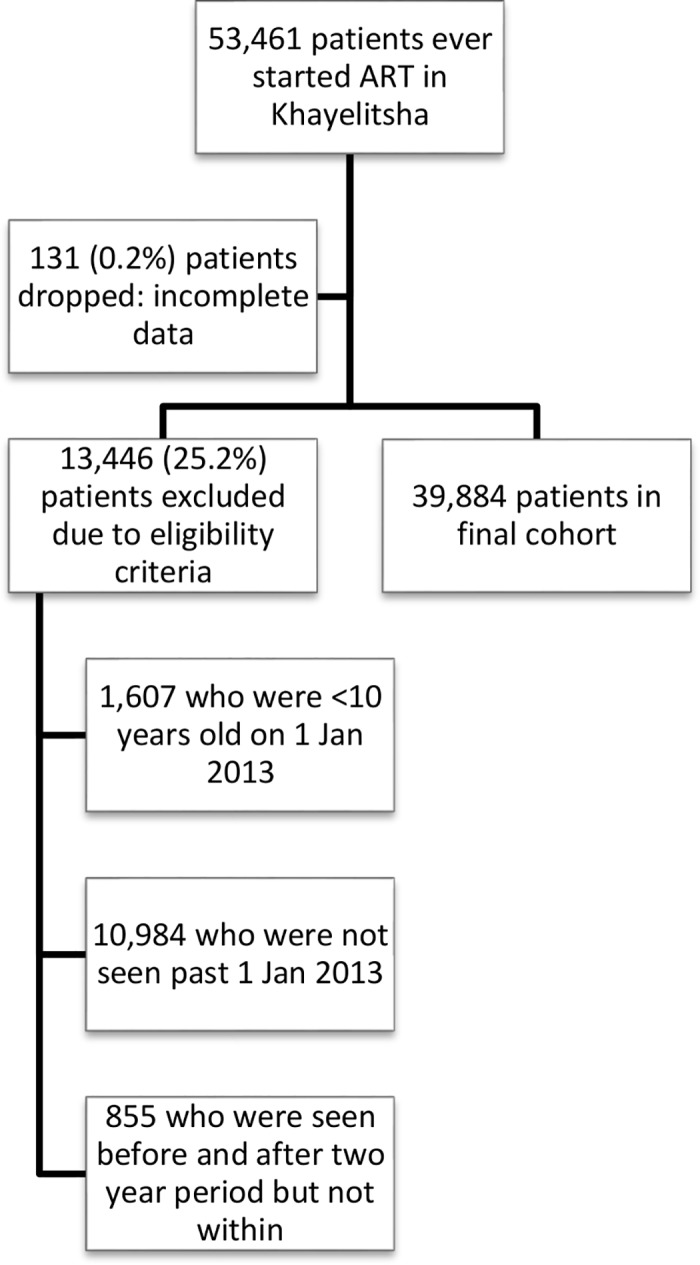
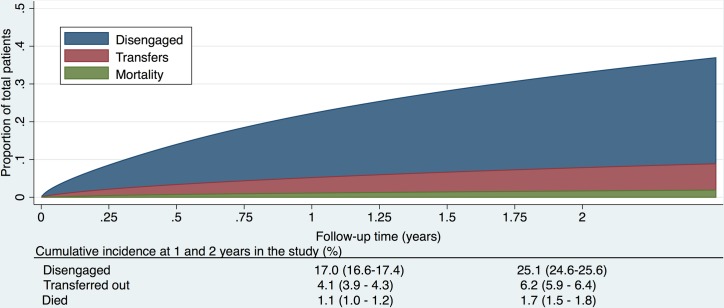
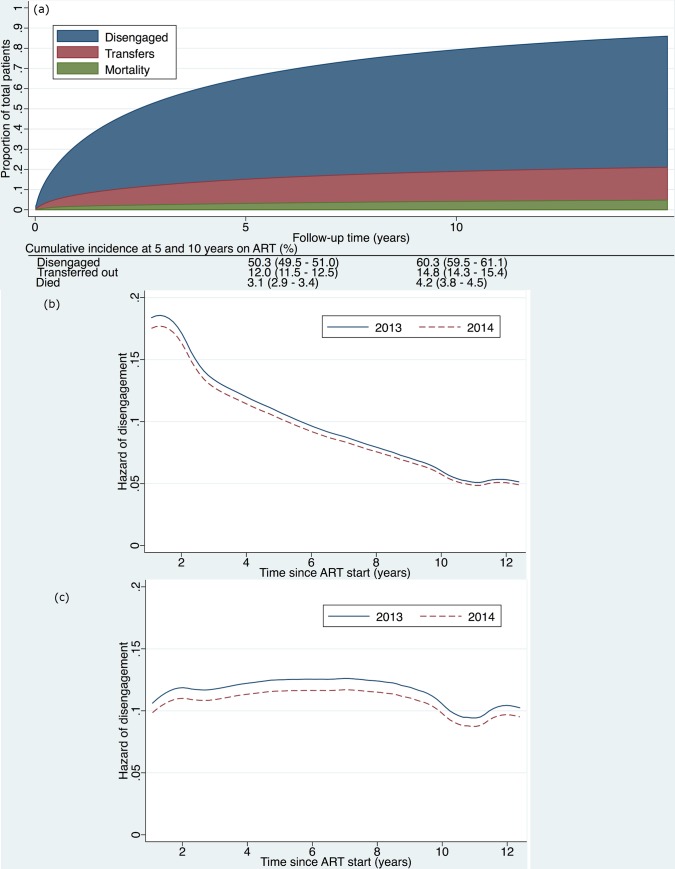
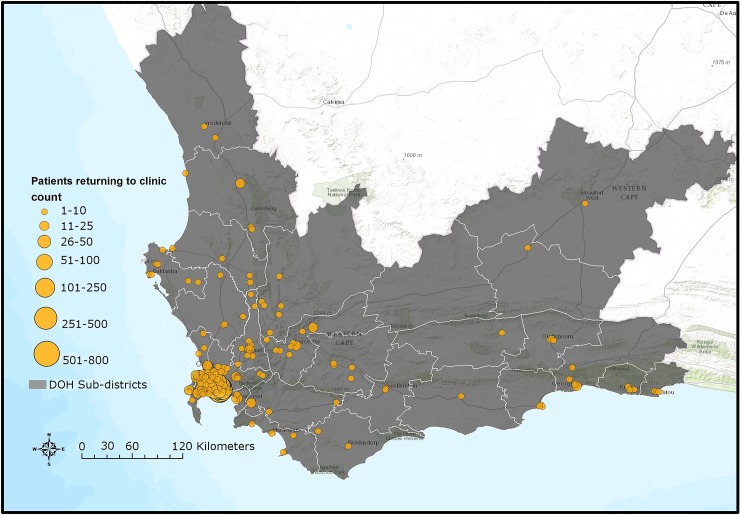
Methods and findings: We conducted a retrospective cohort study of all patients ≥10 years of age who visited 1 of the 13 Khayelitsha ART clinics from 2013-2014 regardless of the date they initiated ART. We described the cumulative incidence of first disengagement (>180 days not attending clinic) between 1 January 2013 and 31 December 2014 using competing risks methods, enabling us to estimate disengagement incidence up to 10 years after ART initiation. We also described risk factors for disengagement based on a Cox proportional hazards model, using multiple imputation for missing data. We ascertained outcomes (death, return to care, hospital admission, other hospital contact, alive but not in care, no information) after disengagement until 30 June 2015 using province-wide health databases and the National Death Registry. Of 39,884 patients meeting our eligibility criteria, the median time on ART to 31 December 2014 was 33.6 months (IQR 12.4-63.2). Of the total study cohort, 592 (1.5%) died in the study period, 1,231 (3.1%) formally transferred out, 987 (2.5%) were silent transfers and visited another Western Cape province clinic within 180 days, 9,005 (22.6%) disengaged, and 28,069 (70.4%) remained in care. Cumulative incidence of disengagement from care was estimated to be 25.1% by 2 years and 50.3% by 5 years on ART. Key factors associated with disengagement (age, male sex, pregnancy at ART start [HR 1.58, 95% CI 1.47-1.69], most recent CD4 count) and retention (ART club membership, baseline CD4) after adjustment were similar to those found in previous studies; however, notably, the higher hazard of disengagement soon after starting ART was no longer present after adjusting for these risk factors. Of the 9,005 who disengaged, the 2 most common initial outcomes were return to ART care after 180 days (33%; n = 2,976) and being alive but not in care in the Western Cape (25%; n = 2,255). After disengagement, a total of 1,459 (16%) patients were hospitalized and 237 (3%) died. The median follow-up from date of disengagement to 30 June 2015 was 16.7 months (IQR 11-22.4). As we included only patient follow-up from 2013-2014 by design in order to maximize the generalizability of our findings to current programs, this limited our ability to more fully describe temporal trends in first disengagement.
Conclusions: Twenty-three percent of ART patients in the large cohort of Khayelitsha, one of the oldest public-sector ART programs in South Africa, disengaged from care at least once in a contemporary 2-year period. Fifty-eight percent of these patients either subsequently returned to care (some "silently") or remained alive without hospitalization, suggesting that many who are considered "lost" actually return to care, and that misclassification of "lost" patients is likely common in similar urban populations. A challenge to meeting ART retention targets is developing, testing, and implementing program designs to target mobile populations and retain them in lifelong care. This should be guided by risk factors for disengagement and improving interlinkage of routine information systems to better support patient care across complex care platforms.
Conflict of interest statement
The authors have read the journal's policy and declare the following competing interests: MO does not have any competing interests that would influence this paper, but does work with the team developing the software used to collect the source data whose guidance and mentorship to the national government are for the benefit of all public health facilities using the software, not just those facilities that are contributing to this paper. This is a non-commercial entity. The other authors have declared that no competing interests exist.
Figures
References
-
- UNAIDS. 90-90-90: An ambitious target to help end the AIDS epidemic 2014. Available from: http://www.unaids.org/en/resources/documents/2014/90-90-90.
-
- Rodger AJ, Cambiano V, Bruun T, Vernazza P, Collins S, van Lunzen J, et al. Sexual activity without condoms and risk of HIV transmission in serodifferent couples when the HIV-positive partner is using suppressive antiretroviral therapy. JAMA. 2016;316(2):171–81. doi: 10.1001/jama.2016.5148 - DOI - PubMed
-
- Stover J, Bollinger L, Izazola JA, Loures L, DeLay P, Ghys PD, et al. What Is Required to End the AIDS Epidemic as a Public Health Threat by 2030? The Cost and Impact of the Fast-Track Approach. PLoS One. 2016;11(5):e0154893 doi: 10.1371/journal.pone.0154893 - DOI - PMC - PubMed
-
- World Health Organization. Global Health Sector Response to HIV, 2000–2015: Focus on Innovations in Africa: Progress report 2015 [updated 2015]. Available from: http://www.who.int/hiv/pub/progressreports/2015-progress-report/en/.
-
- PEPFAR. PEPFAR 2016 Annual Report to Congress 2016. Available from: https://www.pepfar.gov/documents/organization/253940.pdf.
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
