

Expression of p53 protein in high-grade gastroenteropancreatic neuroendocrine carcinoma
- PMID: 29112960
- PMCID: PMC5675414
- DOI: 10.1371/journal.pone.0187667
Expression of p53 protein in high-grade gastroenteropancreatic neuroendocrine carcinoma
Abstract
Background: Gastroenteropancreatic neuroendocrine carcinomas (GEP-NECs) are aggressive, rapidly proliferating tumors. Therapeutic response to current chemotherapy regimens is usually short lasting. The aim of this study was to examine the expression and potential clinical importance of immunoreactive p53 protein in GEP-NEC.
Materials and methods: Tumor tissues from 124 GEP-NEC patients with locally advanced or metastatic disease treated with platinum-based chemotherapy were collected from Nordic centers and clinical data were obtained from the Nordic NEC register. Tumor proliferation rate and differentiation were re-evaluated. All specimens were immunostained for p53 protein using a commercially available monoclonal antibody. Kaplan-Meier curves and cox regression analyses were used to assess progression-free survival (PFS) and overall survival (OS).
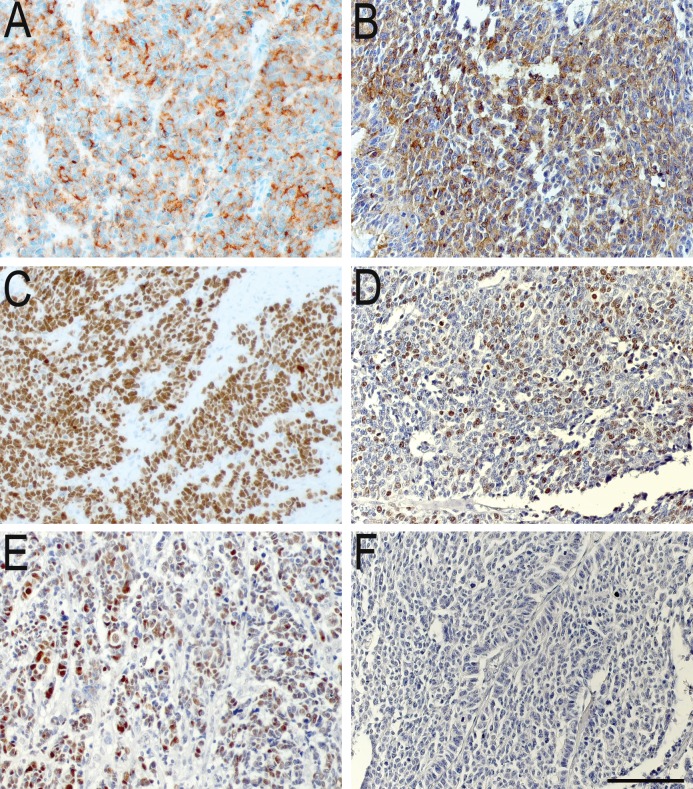
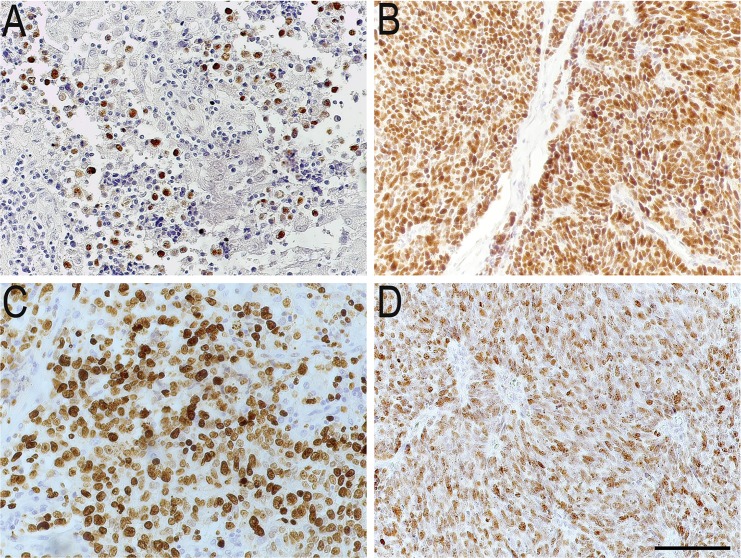
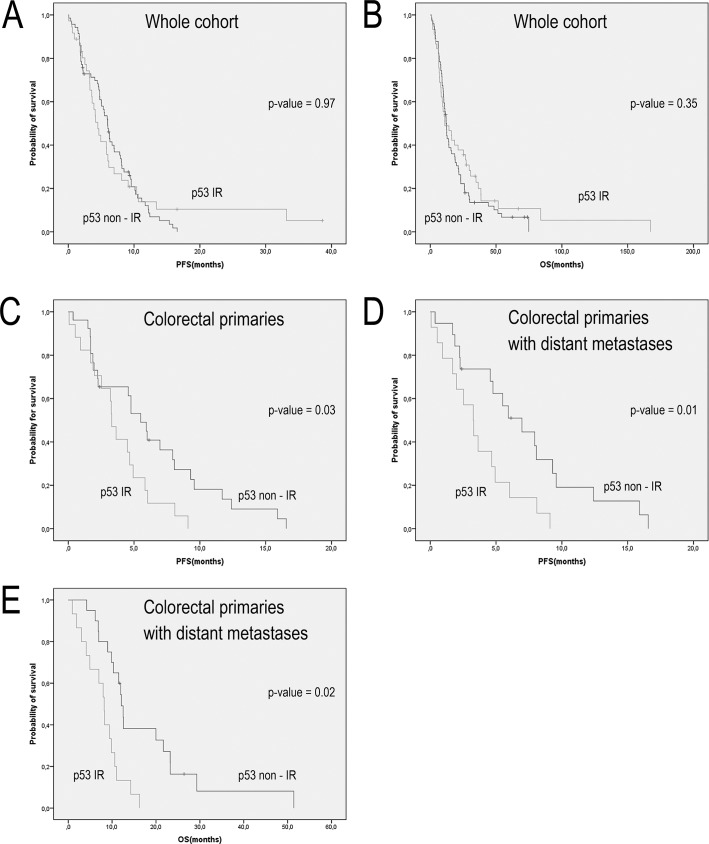
Results: All tumor tissues were immunoreactive for either one or both neuroendocrine biomarkers (chromogranin A and synaptophysin) and Ki67 index was >20% in all cases. p53 immunoreactivity was only shown in 39% of the cases and was not found to be a prognostic marker for the whole cohort. However, p53 immunoreactivity was correlated with shorter PFS in patients with colorectal tumors (HR = 2.1, p = 0.03) in a univariate analysis as well as to poorer PFS (HR = 2.6, p = 0.03) and OS (HR = 3.4, p = 0.02) in patients with colorectal tumors with distant metastases, a correlation which remained significant in the multivariate analyses.
Conclusion: In this cohort of GEP-NEC patients, p53 expression could not be correlated with clinical outcome. However, in patients with colorectal NECs, p53 expression was correlated with shorter PFS and OS. Further studies are needed to establish the role of immunoreactive p53 as a prognostic marker for GEP-NEC patients.
Conflict of interest statement
Figures
References
-
- Bosman FT. World Health Organization., and International Agency for Research on Cancer., WHO classification of tumours of the digestive system 4th ed. World Health Organization classification of tumours. France: Lyon: IARC Press, 2010.; 2010.
-
- Sorbye H, Welin S, Langer SW, Vestermark LW, Holt N, Osterlund P, et al. Predictive and prognostic factors for treatment and survival in 305 patients with advanced gastrointestinal neuroendocrine carcinoma (WHO G3): the NORDIC NEC study. Ann Oncol. 2013;24(1):152–60. Epub 2012/09/13. doi: 10.1093/annonc/mds276 . - DOI - PubMed
-
- Tang LH, Basturk O, Sue JJ, Klimstra DS. A Practical Approach to the Classification of WHO Grade 3 (G3) Well-differentiated Neuroendocrine Tumor (WD-NET) and Poorly Differentiated Neuroendocrine Carcinoma (PD-NEC) of the Pancreas. Am J Surg Pathol. 2016;40(9):1192–202. Epub 2016/06/04. doi: 10.1097/PAS.0000000000000662 ; PubMed Central PMCID: PMC4988129. - DOI - PMC - PubMed
-
- Milione M, Maisonneuve P, Spada F, Pellegrinelli A, Spaggiari P, Albarello L, et al. The Clinicopathologic Heterogeneity of Grade 3 Gastroenteropancreatic Neuroendocrine Neoplasms: Morphological Differentiation and Proliferation Identify Different Prognostic Categories. Neuroendocrinology. 2017;104(1):85–93. Epub 2016/11/03. doi: 10.1159/000445165 . - DOI - PubMed
-
- Sorbye H, Strosberg J, Baudin E, Klimstra DS, Yao JC. Gastroenteropancreatic high-grade neuroendocrine carcinoma. Cancer. 2014;120(18):2814–23. Epub 2014/04/29. doi: 10.1002/cncr.28721 . - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
