

Effects of positive end-expiratory pressure and recruitment maneuvers in a ventilator-induced injury mouse model
- PMID: 29112971
- PMCID: PMC5675408
- DOI: 10.1371/journal.pone.0187419
Effects of positive end-expiratory pressure and recruitment maneuvers in a ventilator-induced injury mouse model
Abstract
Background: Positive-pressure mechanical ventilation is an essential therapeutic intervention, yet it causes the clinical syndrome known as ventilator-induced lung injury. Various lung protective mechanical ventilation strategies have attempted to reduce or prevent ventilator-induced lung injury but few modalities have proven effective. A model that isolates the contribution of mechanical ventilation on the development of acute lung injury is needed to better understand biologic mechanisms that lead to ventilator-induced lung injury.
Objectives: To evaluate the effects of positive end-expiratory pressure and recruitment maneuvers in reducing lung injury in a ventilator-induced lung injury murine model in short- and longer-term ventilation.
Methods: 5-12 week-old female BALB/c mice (n = 85) were anesthetized, placed on mechanical ventilation for either 2 hrs or 4 hrs with either low tidal volume (8 ml/kg) or high tidal volume (15 ml/kg) with or without positive end-expiratory pressure and recruitment maneuvers.
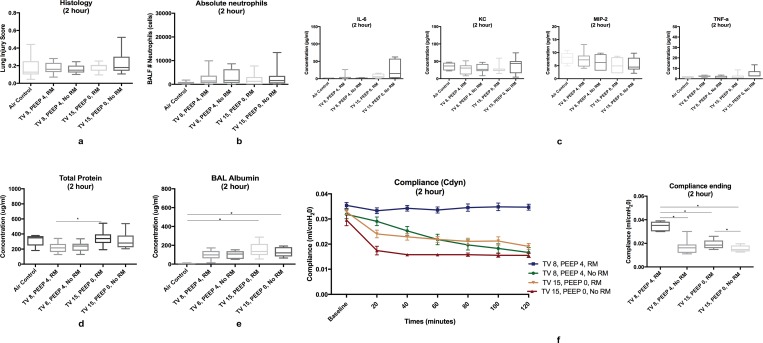
Results: Alteration of the alveolar-capillary barrier was noted at 2 hrs of high tidal volume ventilation. Standardized histology scores, influx of bronchoalveolar lavage albumin, proinflammatory cytokines, and absolute neutrophils were significantly higher in the high-tidal volume ventilation group at 4 hours of ventilation. Application of positive end-expiratory pressure resulted in significantly decreased standardized histology scores and bronchoalveolar absolute neutrophil counts at low- and high-tidal volume ventilation, respectively. Recruitment maneuvers were essential to maintain pulmonary compliance at both 2 and 4 hrs of ventilation.
Conclusions: Signs of ventilator-induced lung injury are evident soon after high tidal volume ventilation (as early as 2 hours) and lung injury worsens with longer-term ventilation (4 hrs). Application of positive end-expiratory pressure and recruitment maneuvers are protective against worsening VILI across all time points. Dynamic compliance can be used guide the frequency of recruitment maneuvers to help ameloriate ventilator-induced lung injury.
Conflict of interest statement
Figures



References
-
- Esteban A, Ferguson ND, Meade MO, Frutos-Vivar F, Apezteguia C, Brochard L, et al. Evolution of mechanical ventilation in response to clinical research. American Journal of Respiratory and Critical Care Medicine. 1777:170–7, 2008. - PubMed
-
- Ware LB, Matthay MA. The acute respiratory distress syndrome. N Engl J Med. May 4;342(18):1334–49, 2000. doi: 10.1056/NEJM200005043421806 - DOI - PubMed
-
- Slutsky AS, Ranieri VM. Ventilator-induced lung injury. N Engl J Med. November 28;369(22):2126–36, 2013. doi: 10.1056/NEJMra1208707 - DOI - PubMed
-
- Curley GF, Laffey JG, Zhang H, Slutsky AS. Biotrauma and Ventilator-Induced Lung Injury: Clinical Implications. Chest. November;150(5):1109–1117, 2016. doi: 10.1016/j.chest.2016.07.019 - DOI - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
