

Squamous cell transformation and EGFR T790M mutation as acquired resistance mechanisms in a patient with lung adenocarcinoma treated with a tyrosine kinase inhibitor: A case report
- PMID: 29113230
- PMCID: PMC5661389
- DOI: 10.3892/ol.2017.6913
Squamous cell transformation and EGFR T790M mutation as acquired resistance mechanisms in a patient with lung adenocarcinoma treated with a tyrosine kinase inhibitor: A case report
Abstract
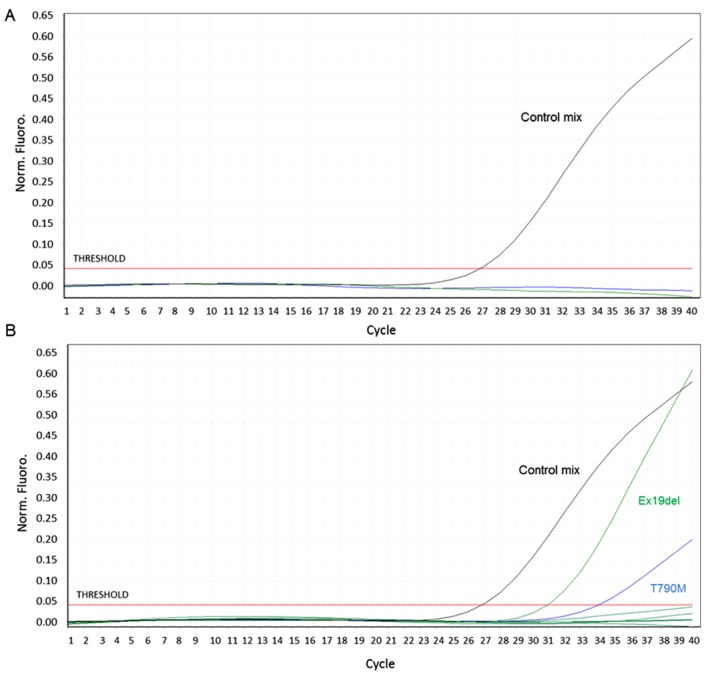
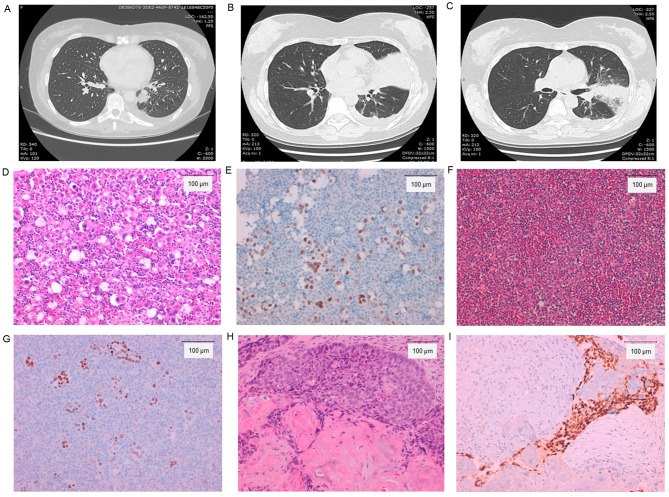
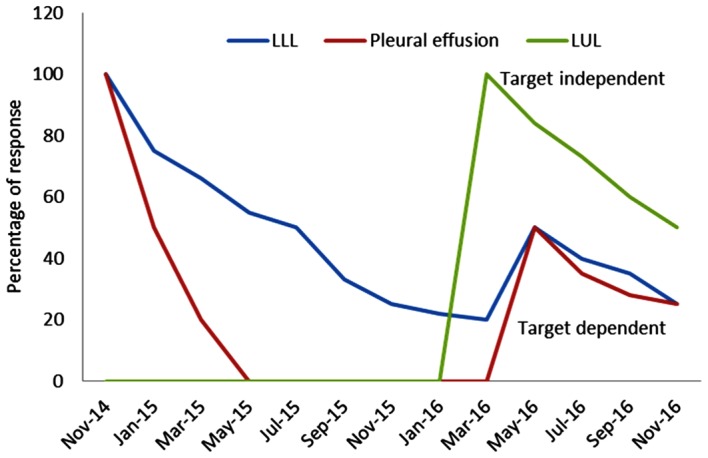
The present case report describes the infrequent coexistence of squamous cell transformation and the epidermal growth factor receptor (EGFR) T790M mutation as resistance mechanisms to first line treatment with tyrosine kinase inhibitors. The patient was a 44-year-old female, diagnosed with a primitive advanced lung adenocarcinoma with bone metastases. The tumor was positive for the EGFR exon 19 deletion, therefore the patient was treated with afatinib (40 mg/day, orally) and radiotherapy for bone lesions. After 16 months, the patient developed resistance. Cytological examination of the pleural effusion confirmed an adenocarcinoma positive for the EGFR exon 19 deletion and the T790M mutation within exon 20, while a biopsy from the upper left bronchus revealed a keratinizing squamous cell carcinoma positive for the EGFR exon 19 deletion. In addition, the EGFR mutations were concomitantly detected in circulating cell-free tumour DNA. Due to the presence of the T790M mutation, the patient underwent osimertinib therapy (80 mg/day, orally), which resulted in a partial tumour regression at the 2-month follow-up, whereas the squamous lesions were treated with radiotherapy. The adenocarcinoma and squamous carcinoma components may share the same origin, according to the presence of the EGFR exon 19 deletion in both lesions. More accurate characterization of resistance mechanisms may lead to the development of improved treatment regimens.
Keywords: epidermal growth factor receptor; lung adenocarcinoma; resistance mechanisms; tyrosine kinase inhibitor.
Figures
References
-
- Rosell R, Carcereny E, Gervais R, Vergnenegre A, Massuti B, Felip E, Palmero R, Garcia-Gomez R, Pallares C, Sanchez JM, et al. Erlotinib versus standard chemotherapy as first-line treatment for European patients with advanced EGFR mutation-positive non-small-cell lung cancer (EURTAC): A multicentre, open-label, randomised phase 3 trial. Lancet Oncol. 2012;13:239–246. doi: 10.1016/S1470-2045(11)70393-X. - DOI - PubMed
-
- Yang JC, Wu YL, Schuler M, Sebastian M, Popat S, Yamamoto N, Zhou C, Hu CP, O'Byrne K, Feng J, et al. Afatinib versus cisplatin-based chemotherapy for EGFR mutation-positive lung adenocarcinoma (LUX-Lung 3 and LUX-Lung 6): Analysis of overall survival data from two randomised, phase 3 trials. Lancet Oncol. 2015;16:141–151. doi: 10.1016/S1470-2045(14)71173-8. - DOI - PubMed
-
- Yu HA, Arcila ME, Rekhtman N, Sima CS, Zakowski MF, Pao W, Kris MG, Miller VA, Ladanyi M, Riely GJ. Analysis of tumour specimens at the time of acquired resistance to EGFR-TKI therapy in 155 patients with EGFR-mutant lung cancers. Clin Cancer Res. 2013;19:2240–2247. doi: 10.1158/1078-0432.CCR-12-2246. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous