

Brain gray matter abnormalities in progressive supranuclear palsy revisited
- PMID: 29113357
- PMCID: PMC5655252
- DOI: 10.18632/oncotarget.20895
Brain gray matter abnormalities in progressive supranuclear palsy revisited
Abstract
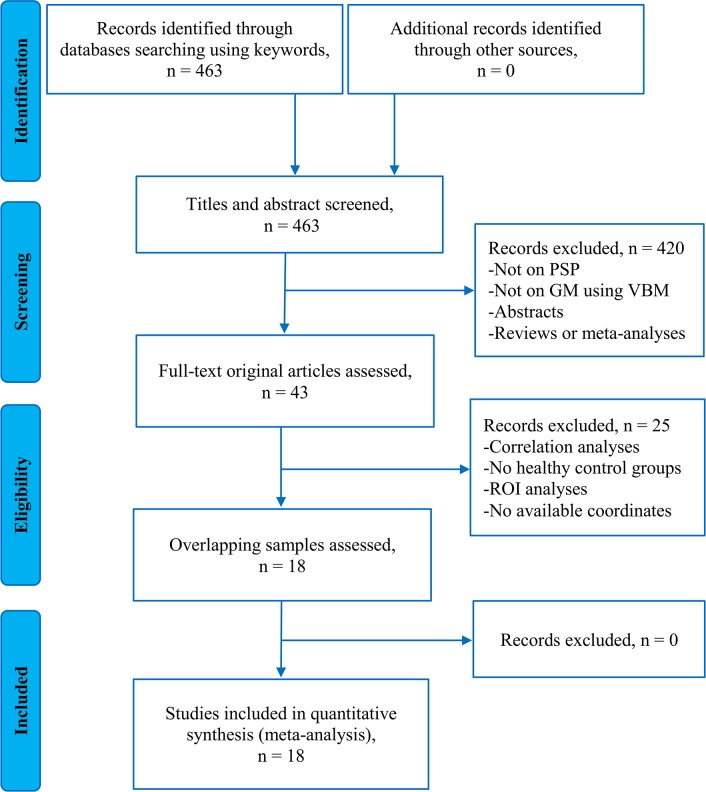
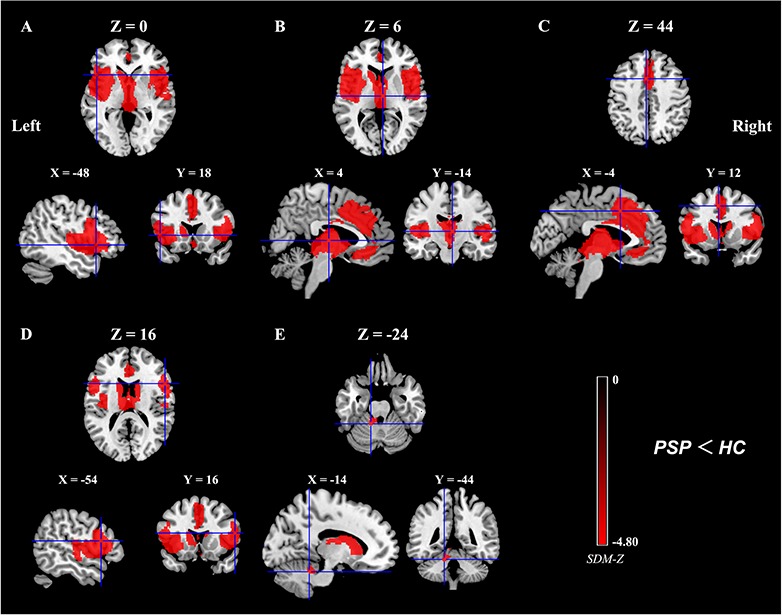
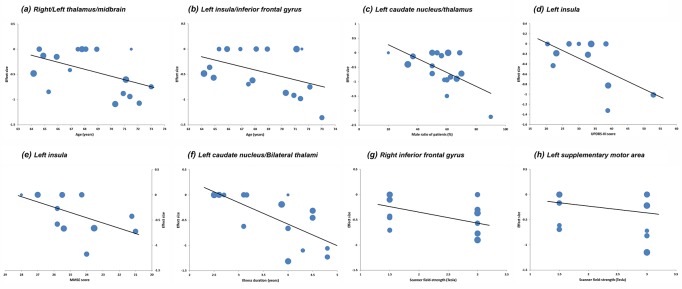
Whole-brain voxel-based morphometry (VBM) studies of progressive supranuclear palsy (PSP) have demonstrated heterogeneous findings regarding gray matter (GM) abnormalities. Here, we used Seed-based d Mapping, a coordinate-based meta-analytic approach to identify consistent regions of GM anomalies across studies of PSP. Totally, 18 original VBM studies, comprising 284 patients with PSP and 367 healthy controls were included. As compared to healthy controls, patients with PSP demonstrated significant GM reductions in both cortical and subcortical regions, including the frontal motor cortices, medial (including anterior cingulate cortex) and lateral frontal cortices, insula, superior temporal gyrus, striatum (putamen and caudate nucleus), thalamus, midbrain, and anterior cerebellum. Our study further suggests that many confounding factors, such as age, male ratio, motor severity, cognitive impairment severity, and illness duration of PSP patients, and scanner field-strength, could contribute to the heterogeneity of GM alterations in PSP across studies. Our comprehensive meta-analysis demonstrates a specific neuroanatomical pattern of GM atrophy in PSP with the involvement of the cortical-subcortical circuitries that mediate vertical supranuclear gaze palsy, motor disabilities (postural instability with falls and parkinsonism), and cognitive-behavioral disturbances. Confounding factors merit attention in future studies.
Keywords: cortical-subcortical circuitries; meta-analysis; progressive supranuclear palsy; seed-based d mapping; voxel-based morphometry.
Conflict of interest statement
CONFLICTS OF INTEREST The authors declare no conflicts of interest.
Figures
Similar articles
-
Voxelwise meta-analysis of gray matter anomalies in progressive supranuclear palsy and Parkinson's disease using anatomic likelihood estimation.Front Hum Neurosci. 2014 Feb 18;8:63. doi: 10.3389/fnhum.2014.00063. eCollection 2014. Front Hum Neurosci. 2014. PMID: 24600372 Free PMC article.
-
Atrophy in midbrain & cerebral/cerebellar pedunculi is characteristic for progressive supranuclear palsy - A double-validation whole-brain meta-analysis.Neuroimage Clin. 2019;22:101722. doi: 10.1016/j.nicl.2019.101722. Epub 2019 Feb 19. Neuroimage Clin. 2019. PMID: 30831462 Free PMC article.
-
A voxel based comparative analysis using magnetization transfer imaging and T1-weighted magnetic resonance imaging in progressive supranuclear palsy.Ann Indian Acad Neurol. 2014 Apr;17(2):193-8. doi: 10.4103/0972-2327.132626. Ann Indian Acad Neurol. 2014. PMID: 25024571 Free PMC article.
-
Gray matter atrophy in progressive supranuclear palsy: meta-analysis of voxel-based morphometry studies.Neurol Sci. 2013 Jul;34(7):1049-55. doi: 10.1007/s10072-013-1406-9. Epub 2013 Mar 30. Neurol Sci. 2013. PMID: 23543378 Review.
-
Advanced structural neuroimaging in progressive supranuclear palsy: Where do we stand?Parkinsonism Relat Disord. 2017 Mar;36:19-32. doi: 10.1016/j.parkreldis.2016.12.023. Epub 2016 Dec 26. Parkinsonism Relat Disord. 2017. PMID: 28057431 Review.
Cited by
-
The Role of MicroRNAs in Progressive Supranuclear Palsy-A Systematic Review.Int J Mol Sci. 2024 Jul 28;25(15):8243. doi: 10.3390/ijms25158243. Int J Mol Sci. 2024. PMID: 39125813 Free PMC article.
-
Schizotypal traits across the amyotrophic lateral sclerosis-frontotemporal dementia spectrum: pathomechanistic insights.J Neurol. 2022 Aug;269(8):4241-4252. doi: 10.1007/s00415-022-11049-3. Epub 2022 Mar 13. J Neurol. 2022. PMID: 35279757 Free PMC article.
-
The Spectrum of Cognitive Impairment in Atypical Parkinsonism Syndromes: A Comprehensive Review of Current Understanding and Research.Diseases. 2025 Jan 31;13(2):39. doi: 10.3390/diseases13020039. Diseases. 2025. PMID: 39997046 Free PMC article. Review.
-
Cerebellar contributions to cognition in corticobasal syndrome and progressive supranuclear palsy.Brain Commun. 2020 Nov 16;2(2):fcaa194. doi: 10.1093/braincomms/fcaa194. eCollection 2020. Brain Commun. 2020. PMID: 33381758 Free PMC article.
-
Pathomechanisms of cognitive impairment in progressive supranuclear palsy.J Neural Transm (Vienna). 2023 Apr;130(4):481-493. doi: 10.1007/s00702-023-02613-w. Epub 2023 Mar 2. J Neural Transm (Vienna). 2023. PMID: 36862189 Review.
References
-
- Williams DR, de Silva R, Paviour DC, Pittman A, Watt HC, Kilford L, Holton JL, Revesz T, Lees AJ. Characteristics of two distinct clinical phenotypes in pathologically proven progressive supranuclear palsy: Richardson's syndrome and PSP-parkinsonism. Brain. 2005;128:1247–58. https://doi.org/10.1093/brain/awh488 - DOI - PubMed
-
- Kansal K, Mareddy M, Sloane KL, Minc AA, Rabins PV, McGready JB, Onyike CU. Survival in Frontotemporal Dementia Phenotypes: A Meta-Analysis. Dement Geriatr Cogn Disord. 2016;41:109–22. https://doi.org/10.1159/000443205 - DOI - PubMed
-
- Williams DR, Lees AJ. Progressive supranuclear palsy: clinicopathological concepts and diagnostic challenges. Lancet Neurol. 2009;8:270–9. https://doi.org/10.1016/s1474-4422(09)70042-0 - DOI - PubMed
-
- Josephs KA. Key emerging issues in progressive supranuclear palsy and corticobasal degeneration. J Neurol. 2015;262:783–8. https://doi.org/10.1007/s00415-015-7682-y - DOI - PMC - PubMed
-
- Steele JC, Richardson JC, Olszewski J. progressive supranuclear palsy. a heterogeneous degeneration involving the brain stem, basal ganglia and cerebellum with vertical gaze and pseudobulbar palsy, nuchal dystonia and dementia. Arch Neurol. 1964;10:333–59. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
