

Magnetic Resonance Imaging Appearance of Schwannomas from Head to Toe: A Pictorial Review
- PMID: 29114437
- PMCID: PMC5651654
- DOI: 10.4103/jcis.JCIS_40_17
Magnetic Resonance Imaging Appearance of Schwannomas from Head to Toe: A Pictorial Review
Abstract
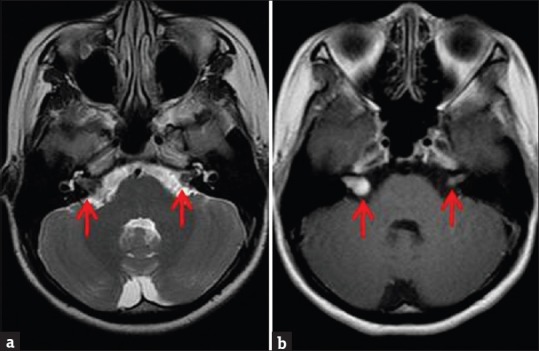
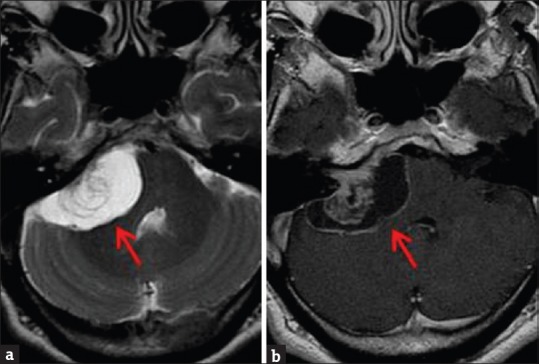
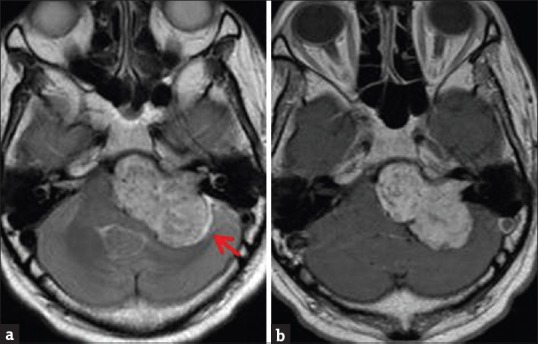
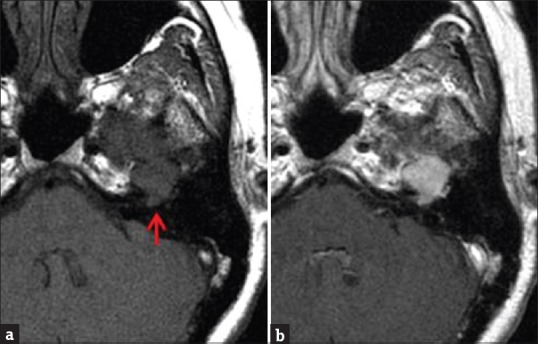
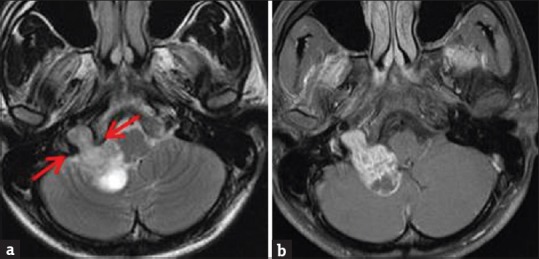
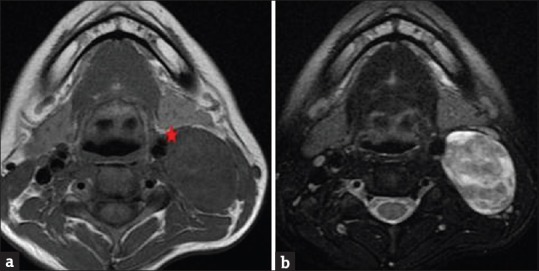
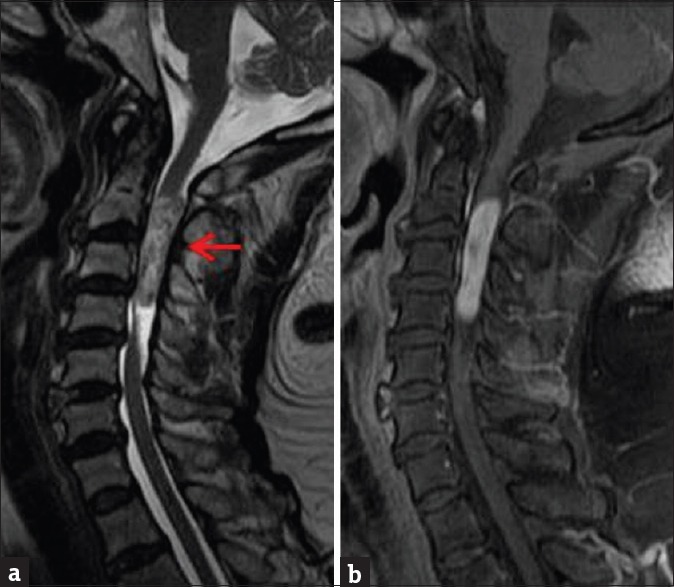
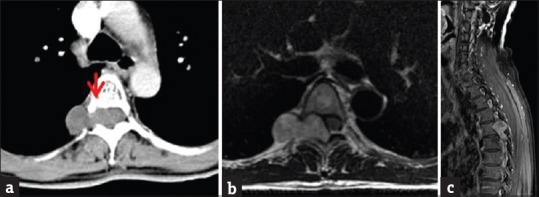
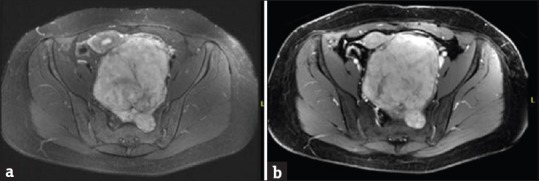
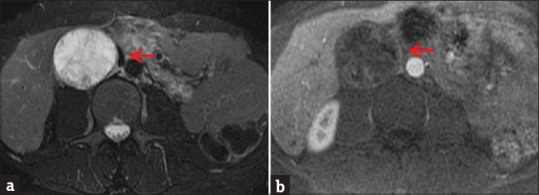
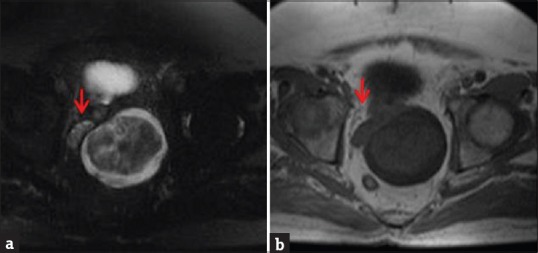
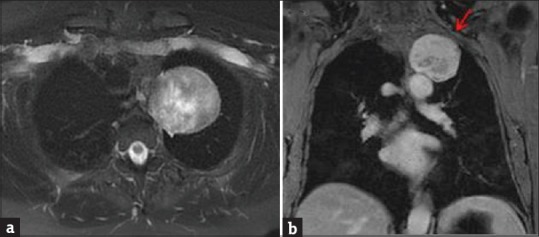
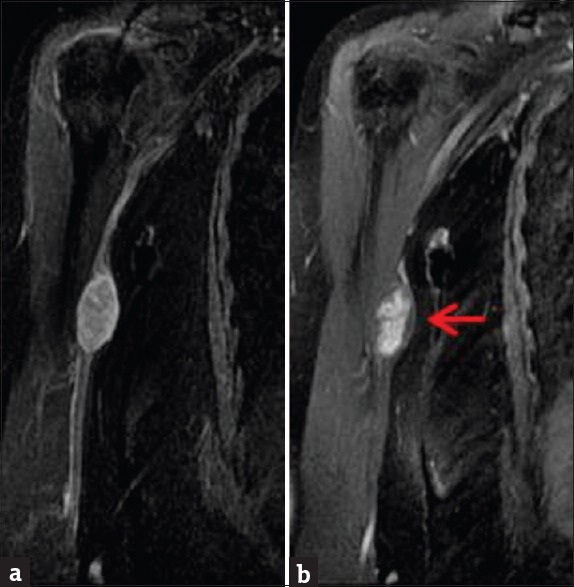
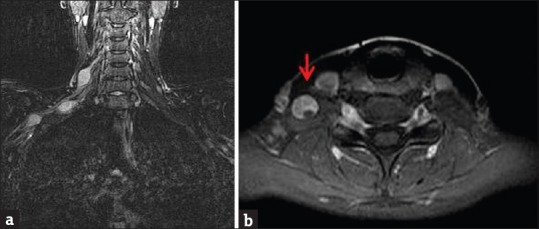
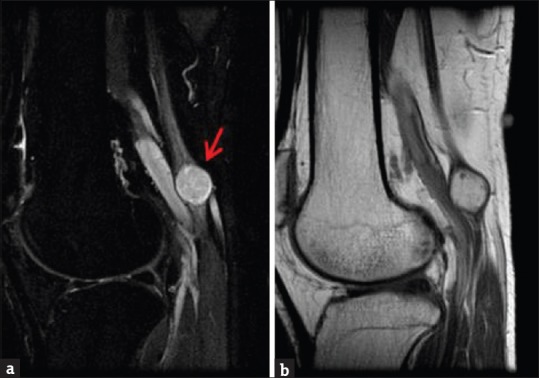
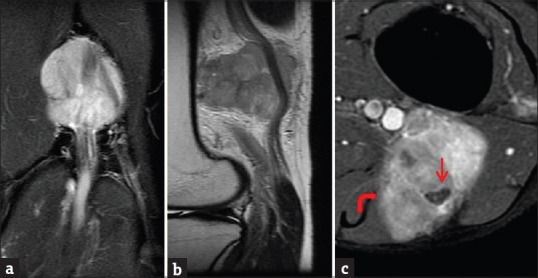
Schwannomas are benign soft-tissue tumors that arise from peripheral nerve sheaths throughout the body and are commonly encountered in patients with neurofibromatosis Type 2. The vast majority of schwannomas are benign, with rare cases of malignant transformation reported. In this pictorial review, we discuss the magnetic resonance imaging (MRI) appearance of schwannomas by demonstrating a collection of tumors from different parts of the body that exhibit similar MRI characteristics. We review strategies to distinguish schwannomas from malignant soft-tissue tumors while exploring the anatomic and histologic origins of these tumors to discuss how this correlates with their imaging findings. Familiarity with the MRI appearance of schwannomas can help aid in the differential diagnosis of soft-tissue masses, especially in unexpected locations.
Keywords: Magnetic resonance imaging; malignant peripheral nerve sheath tumor; peripheral nerve sheath tumor; schwannoma.
Conflict of interest statement
There are no conflicts of interest.
Figures


References
-
- Murphey MD, Smith WS, Smith SE, Kransdorf MJ, Temple HT. From the archives of the AFIP. Imaging of musculoskeletal neurogenic tumors: Radiologic-pathologic correlation. Radiographics. 1999;19:1253–80. - PubMed
-
- Gomez-Brouchet A, Delisle MB, Cognard C, Bonafe A, Charlet JP, Deguine O, et al. Vestibular schwannomas: Correlations between magnetic resonance imaging and histopathologic appearance. Otol Neurotol. 2001;22:79–86. - PubMed
-
- Moukarbel RV, Sabri AN. Current management of head and neck schwannomas. Curr Opin Otolaryngol Head Neck Surg. 2005;13:117–22. - PubMed
-
- Parmar HA, Ibrahim M, Castillo M, Mukherji SK. Pictorial essay: Diverse imaging features of spinal schwannomas. J Comput Assist Tomogr. 2007;31:329–34. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials