

Molecular diagnostics of lung cancer in the clinic
- PMID: 29114472
- PMCID: PMC5653520
- DOI: 10.21037/tlcr.2017.08.03
Molecular diagnostics of lung cancer in the clinic
Abstract
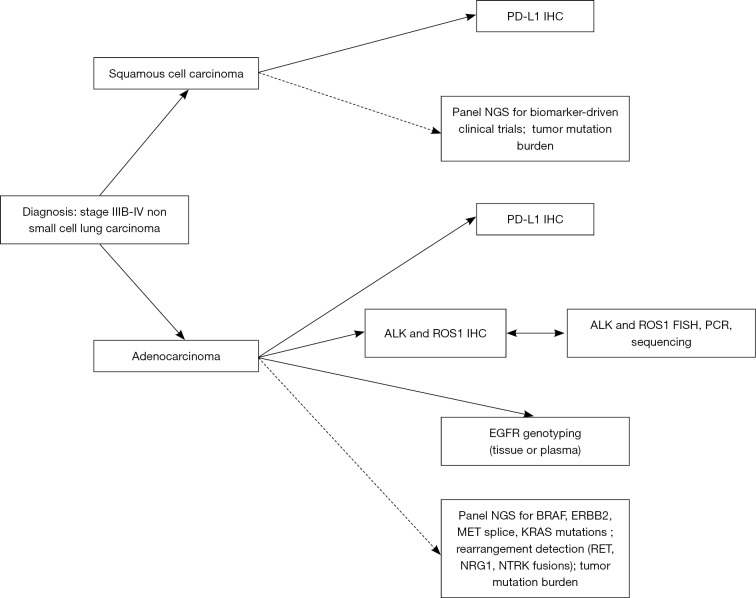
According to current practice guidelines, all patients with advanced non-small cell lung cancer (NSCLC) should undergo predictive biomarker testing. For squamous cell carcinoma patients, PD-L1 immunohistochemistry is indicated to select patients for immunotherapy in the first line. For lung adenocarcinoma, all patients with advanced disease should undergo testing for epidermal growth factor receptor (EGFR) mutations, ALK and ROS1 rearrangements, and PD-L1 expression to predict response to EGFR, ALK, or ROS1 targeted inhibitors or immunotherapy, respectively. Besides these, a number of other biomarkers are under clinical investigation as predictors of response to targeted therapies, including BRAF, ERBB2, MET splice mutations and amplification, and RET rearrangements. Successful testing for this complex array of molecular targets demands careful coordination between proceduralists, pathologists and molecular laboratories to ensure proper tumor tissue handling following biopsy as well as judicious use of diagnostic immunohistochemistry. Even so, sample failure rates due to inadequate tumor tissue are high in practice, particularly when using sequential testing methods. Use of next generation sequencing (NGS) in clinical practice can enable detection of multiple targets and multiple alteration types (mutation, gene copy change, and rearrangement) simultaneously even with small amounts of input nucleic acids, thus increasing molecular testing success rates. In patients with an established lung cancer diagnosis but with prohibitively limited amounts of tumor tissue or who are experiencing relapse, analyses of circulating tumor DNA (ctDNA) from the plasma can serve as an alternate testing substrate, however the more limited clinical sensitivity of this approach must be taken into account. This review will explore the indications for and pitfalls of routine NGS and plasma genotyping in the clinic, including the intersection of these technologies.
Keywords: ALK; Epidermal growth factor receptor (EGFR); ROS1; circulating tumor DNA (ctDNA); lung adenocarcinoma; next generation sequencing (NGS); plasma genotyping.
Conflict of interest statement
Conflicts of Interest: The author has no conflicts of interest to declare.
Figures

References
-
- Cancer Stat Facts: Lung and Bronchus Cancer. Available online: https://seer.cancer.gov/statfacts/html/lungb.html
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous