Test-retest reliability of repeated knee laxity measurements in the acute phase following a knee trauma using a Rolimeter
- PMID: 29114530
- PMCID: PMC5667602
- DOI: 10.12965/jer.1735104.552
Test-retest reliability of repeated knee laxity measurements in the acute phase following a knee trauma using a Rolimeter
Abstract
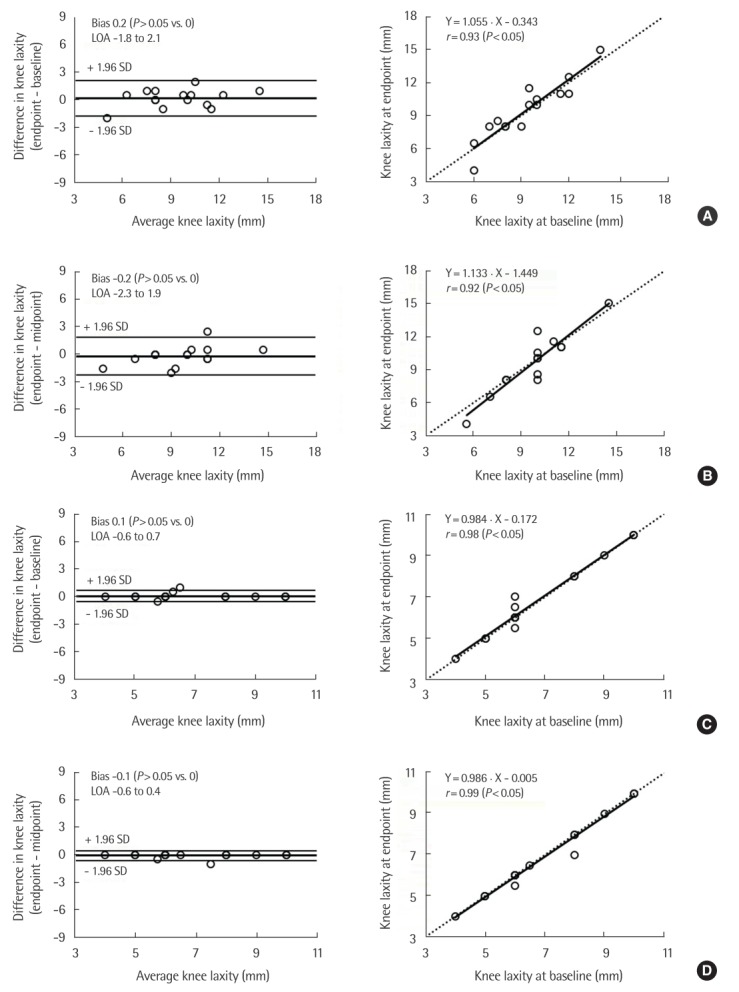
The purpose was to examine the test-retest reliability of the Rolimeter measurement procedure in the acute time phase, following a substantial knee trauma. In total, 15 participants with acute knee trauma were examined by one single observer at three different time-points with the Rolimeter using a maximum force. The selected time-points were: baseline (0-7 days after the trauma), midpoint (3-4 weeks after the trauma), and endpoint (3-4 weeks after the trauma). The anterior-posterior displacement was recorded where the endpoint evaluation was used as the reference value. The mean anterior laxity scores remained constant over the measurement time-points for both knees, with an anterior laxity that was 2.7 mm higher (on average) in the injured than the noninjured knee (9.5 mm vs. 6.8 mm). The mean difference (i.e., bias) between laxity scores, for the injured knee, measured at endpoint versus baseline was 0.2±1.0 mm and -0.2±1.1 mm when measured at endpoint versus midpoint, with average typical errors of 0.7 and 0.8 mm and intra-class correlations that were very strong (both r=~0.93). For the same comparisons on the noninjured knee, systematic bias was close to zero (0.1±0.3 and -0.1±0.3 mm, respectively), and both the intra-class correlations were almost perfect (r=~0.99). The current study implicates that repeated Rolimeter measurements are relatively reliable for quantifying anterior knee laxity during the acute time-phases following knee trauma. Hence, the Rolimeter, in combination with manual tests, seems to be a valuable tool for identifying anterior cruciate ligament injuries.
Keywords: Anterior cruciate ligament; Arthrometer; Hemarthrosis; Instability; Knee joint.
Conflict of interest statement
CONFLICT OF INTEREST No potential conflict of interest relevant to this article was reported.
Figures


References
-
- Balasch H, Schiller M, Friebel H, Hoffmann F. Evaluation of anterior knee joint instability with the Rolimeter. A test in comparison with manual assessment and measuring with the KT-1000 arthrometer. Knee Surg Sports Traumatol Arthrosc. 1999;7:204–208. - PubMed
-
- Benjaminse A, Gokeler A, van der Schans CP. Clinical diagnosis of an anterior cruciate ligament rupture: a meta-analysis. J Orthop Sports Phys Ther. 2006;36:267–288. - PubMed
-
- Bland JM, Altman DG. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet. 1986;1:307–310. - PubMed
-
- Bollen SR, Scott BW. Rupture of the anterior cruciate ligament: a quiet epidemic? Injury. 1996;27:407–409. - PubMed
-
- Daniel DM, Stone ML, Sachs R, Malcom L. Instrumented measurement of anterior knee laxity in patients with acute anterior cruciate ligament disruption. Am J Sports Med. 1985;13:401–407. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources