

Oncological outcomes from trimodality therapy receiving definitive doses of neoadjuvant chemoradiation (≥60 Gy) and factors influencing consideration for surgery in stage III non-small cell lung cancer
- PMID: 29114590
- PMCID: PMC5605306
- DOI: 10.1016/j.adro.2017.07.009
Oncological outcomes from trimodality therapy receiving definitive doses of neoadjuvant chemoradiation (≥60 Gy) and factors influencing consideration for surgery in stage III non-small cell lung cancer
Abstract
Purpose: Guidelines for locally advanced non-small cell lung cancer (LA-NSCLC) recommend definitive chemoradiation therapy (CRT) for cN2-N3 disease, reserving surgery for patients with minimal nodal involvement at presentation. The current literature suggests that surgery after CRT for stage III NSCLC can improve freedom-from-recurrence (FFR) but has not consistently demonstrated an improvement in overall survival, perhaps partly due to the low (45-50.4 Gy) preoperative doses delivered that result in low rates of mediastinal nodal clearance. We therefore analyzed factors associated with trimodality therapy receipt and determined outcomes in patients with LA-NSCLC who were treated with definitive doses (≥60 Gy) of neoadjuvant CRT prior to surgery.
Methods and materials: We retrospectively analyzed 355 consecutive patients with LA-NSCLC who were treated with curative intent between January 2000 and December 2013. The Kaplan-Meier method was used to estimate the overall survival and FFR of patients who were initially planned to receive trimodality treatment but never underwent surgery (unplanned bimodality) compared with those who were never considered to be surgical candidates (planned bimodality) and those who underwent surgical resection after CRT (trimodality). Cox proportional hazards regression with forward selection was used for multivariate analyses, and the Fisher exact test was used to test contingency tables.
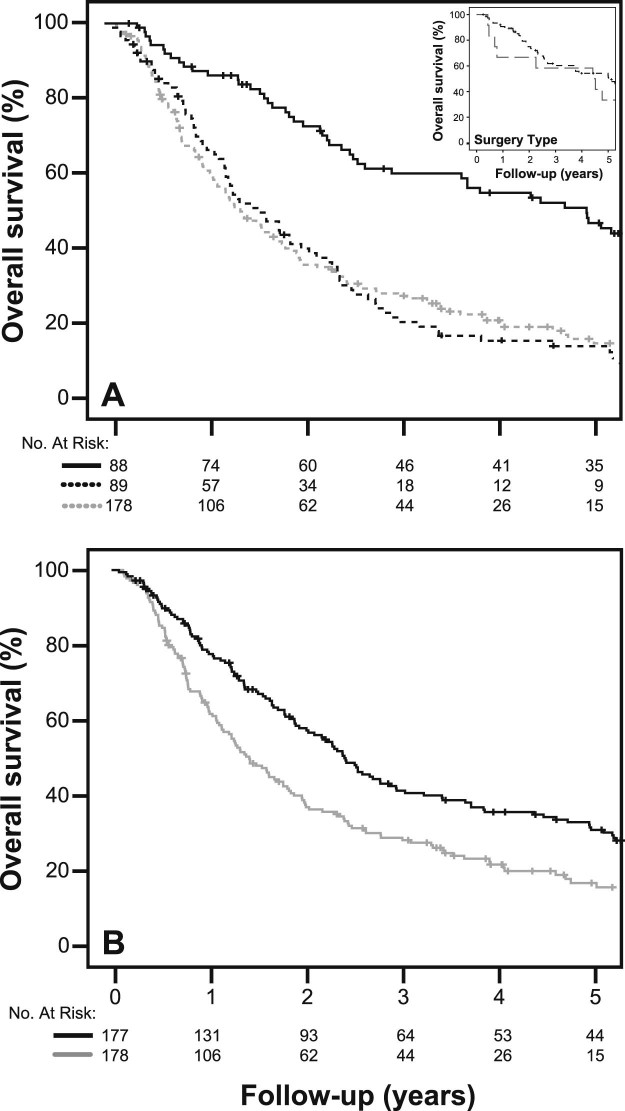
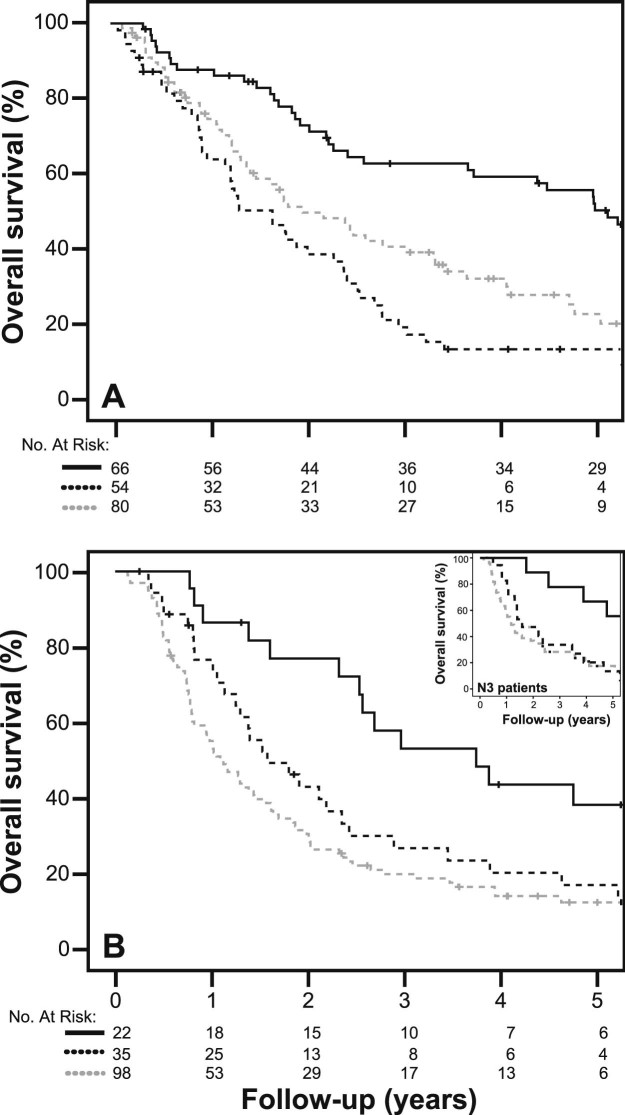
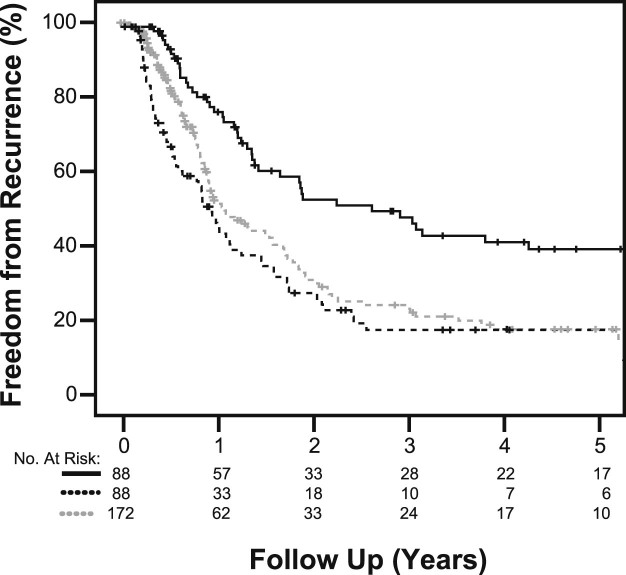
Results: Patients who received trimodality therapy had a longer median survival than those with unplanned or planned bimodality therapy at 59.9, 20.1, and 17.3 months, respectively (P < .001). The survival benefit with surgery persisted in patients with stage IIIB (P < .001) and N3 (P = .010) nodal disease when mediastinal nodal clearance was achieved. FFR was also improved with surgical resection (P = .001). Race (P < .001), stage (P < .001), performance status (P < .001), age (P < .001), and diagnosis of chronic obstructive pulmonary disease (P = .009) were significant indicators that influenced both the decision to initially choose trimodality therapy at consultation and to actually perform surgical resection.
Conclusions: Trimodality treatment significantly improves survival and FFR in patients with LA-NSCLC when definitive doses of radiation with neoadjuvant chemotherapy are employed. We identified important demographic features that predict the use of surgical intervention in patients with stage III NSCLC.
Figures
Similar articles
-
Implications of Pathologic Complete Response Beyond Mediastinal Nodal Clearance With High-Dose Neoadjuvant Chemoradiation Therapy in Locally Advanced, Non-Small Cell Lung Cancer.Int J Radiat Oncol Biol Phys. 2018 Jun 1;101(2):445-452. doi: 10.1016/j.ijrobp.2018.02.003. Epub 2018 Feb 13. Int J Radiat Oncol Biol Phys. 2018. PMID: 29559292
-
'CROSS'-ing into the 'Real World': a retrospective cohort study of patients receiving trimodality and bimodality therapy for esophageal cancer.J Gastrointest Oncol. 2023 Apr 29;14(2):480-493. doi: 10.21037/jgo-22-633. Epub 2023 Apr 24. J Gastrointest Oncol. 2023. PMID: 37201058 Free PMC article.
-
Clinical outcomes of black vs. non-black patients with locally advanced non-small cell lung cancer.Lung Cancer. 2017 Dec;114:44-49. doi: 10.1016/j.lungcan.2017.10.016. Epub 2017 Nov 2. Lung Cancer. 2017. PMID: 29173764
-
Patterns of failure following surgical resection for malignant pleural mesothelioma.Thorac Surg Clin. 2004 Nov;14(4):567-73. doi: 10.1016/j.thorsurg.2004.06.006. Thorac Surg Clin. 2004. PMID: 15559064 Review.
-
Surgery after chemoradiotherapy in patients with stage III (N2 or N3, excluding T4) non-small-cell lung cancer: a systematic review.Curr Oncol. 2019 Jun;26(3):e398-e404. doi: 10.3747/co.26.4549. Epub 2019 Jun 1. Curr Oncol. 2019. PMID: 31285684 Free PMC article.
Cited by
-
Resectable IIIA-N2 Non-Small-Cell Lung Cancer (NSCLC): In Search for the Proper Treatment.Cancers (Basel). 2020 Jul 25;12(8):2050. doi: 10.3390/cancers12082050. Cancers (Basel). 2020. PMID: 32722386 Free PMC article. Review.
-
Optimal surgical timing and radiotherapy dose for trimodality therapy in locally advanced non-small cell lung cancer.Cancer Med. 2021 Sep;10(17):5794-5808. doi: 10.1002/cam4.4123. Epub 2021 Aug 5. Cancer Med. 2021. PMID: 34350713 Free PMC article.
-
Reirradiation for locoregionally recurrent non-small cell lung cancer.J Thorac Dis. 2018 Aug;10(Suppl 21):S2522-S2536. doi: 10.21037/jtd.2017.12.50. J Thorac Dis. 2018. PMID: 30206496 Free PMC article. Review.
-
Surgical complications and clinical outcomes after dose-escalated trimodality therapy for non-small cell lung cancer in the era of intensity-modulated radiotherapy.Radiother Oncol. 2021 Dec;165:44-51. doi: 10.1016/j.radonc.2021.10.012. Epub 2021 Oct 22. Radiother Oncol. 2021. PMID: 34695520 Free PMC article.
-
Contemporary Strategies: Incorporating Immunotherapy into Stage 3 Non-small Cell Lung Cancer Treatment.Tuberc Respir Dis (Seoul). 2024 Jul;87(3):292-301. doi: 10.4046/trd.2023.0162. Epub 2024 Mar 28. Tuberc Respir Dis (Seoul). 2024. PMID: 38547860 Free PMC article.
References
-
- Siegel R.L., Miller K.D., Jemal A. Cancer statistics, 2016. CA Cancer J Clin. 2016;66:7–30. - PubMed
-
- Goldstraw P., Chansky K., Crowley J. The IASLC lung cancer staging project: Proposals for revision of the TNM stage groupings in the forthcoming (eighth) edition of the TNM Classification for lung cancer. J Thorac Oncol. 2016;11:39–51. - PubMed
-
- Varlotto J.M., Yao A.N., DeCamp M.M. Nodal stage of surgically resected non-small cell lung cancer and its effect on recurrence patterns and overall survival. Int J Radiat Oncol Biol Phys. 2015;91:765–773. - PubMed
-
- Watanabe Y., Hayashi Y., Shimizu J., Oda M., Iwa T. Mediastinal nodal involvement and the prognosis of non-small cell lung cancer. Chest. 1991;100:422–428. - PubMed
-
- Sakao Y., Miyamoto H., Yamazaki A. Prognostic significance of metastasis to the highest mediastinal lymph node in nonsmall cell lung cancer. Ann Thorac Surg. 2006;81:292–297. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
